

Is duodeno-jejunal bypass liner superior to pylorus preserving bariatric surgery in terms of complications and efficacy?
- PMID: 33712874
- PMCID: PMC8370966
- DOI: 10.1007/s00423-021-02131-x
Is duodeno-jejunal bypass liner superior to pylorus preserving bariatric surgery in terms of complications and efficacy?
Abstract
Purpose: Based on recent scientific evidence, bariatric surgery is more effective in the management of morbid obesity and related comorbidities than conservative therapy. Pylorus preserving surgical procedures (PPBS) such as laparoscopic single-anastomosis duodeno-jejunal or duodeno-ileal bypass with sleeve gastrectomy are modified duodenal switch (DS) surgical techniques. The duodeno-jejunal bypass liner (DJBL) is a novel surgical method in the inventory of metabolism focused manual interventions that excludes duodeno-jejunal mucosa from digestion, mimicking DS procedures without the risk of surgical intervention. The aim of this article is to summarize and compare differences between safety-related features and weight loss outcomes of DJBL and PPBS.
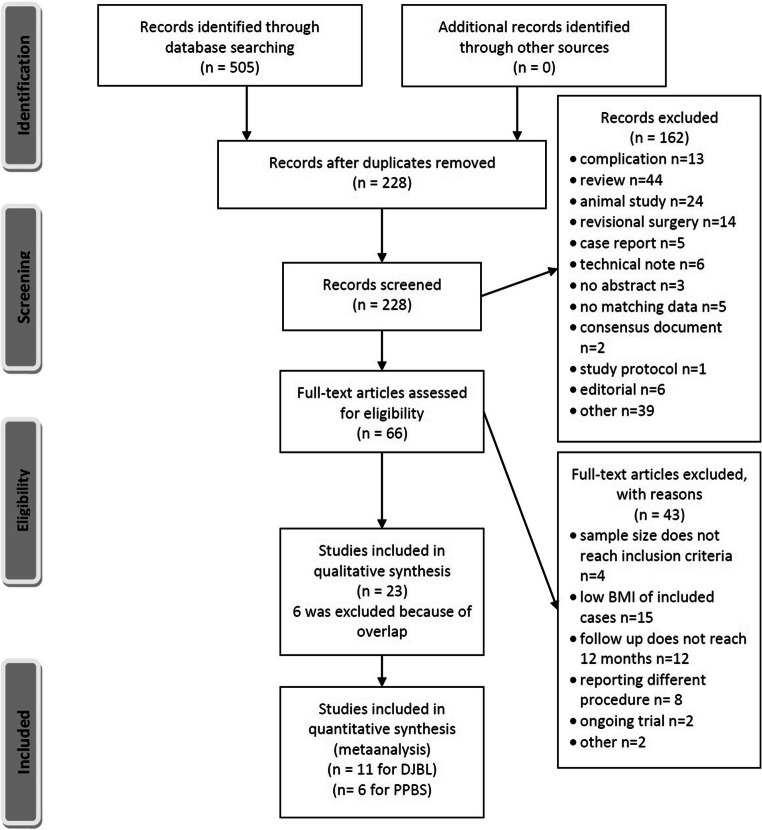
Methods: A literature search was conducted in the PubMed database. Records of DJBL-related adverse events (AEs), occurrence of PPBS-related complications and reintervention rates were collected. Mean weight, mean body mass index (BMI), percent of excess of weight loss (EWL%), percent of total weight loss (TWL%) and BMI value alterations were recorded for weight loss outcomes.
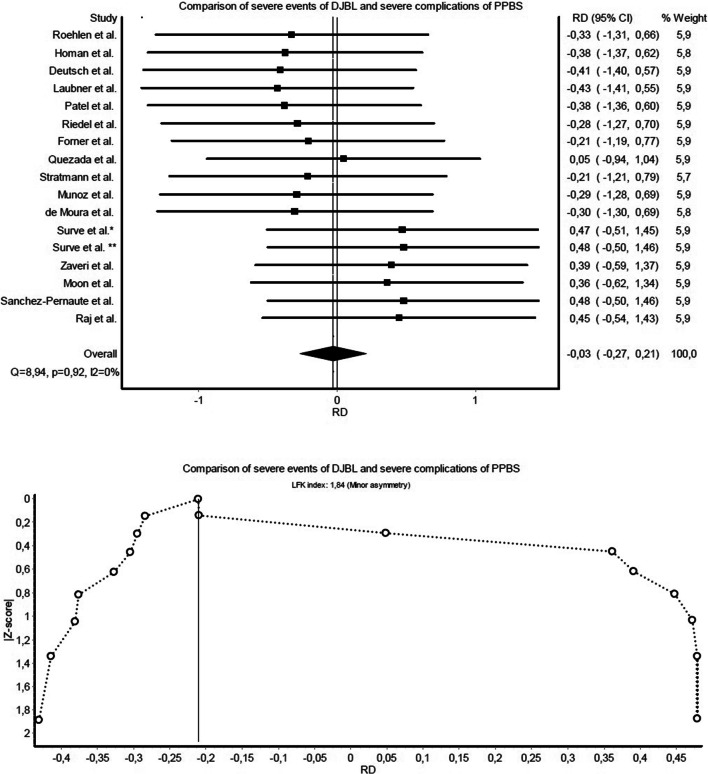
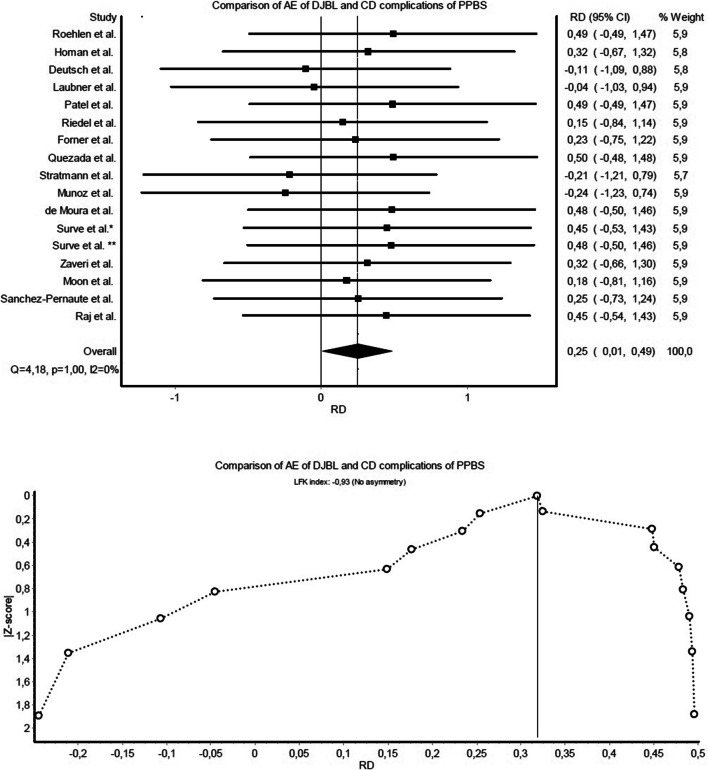
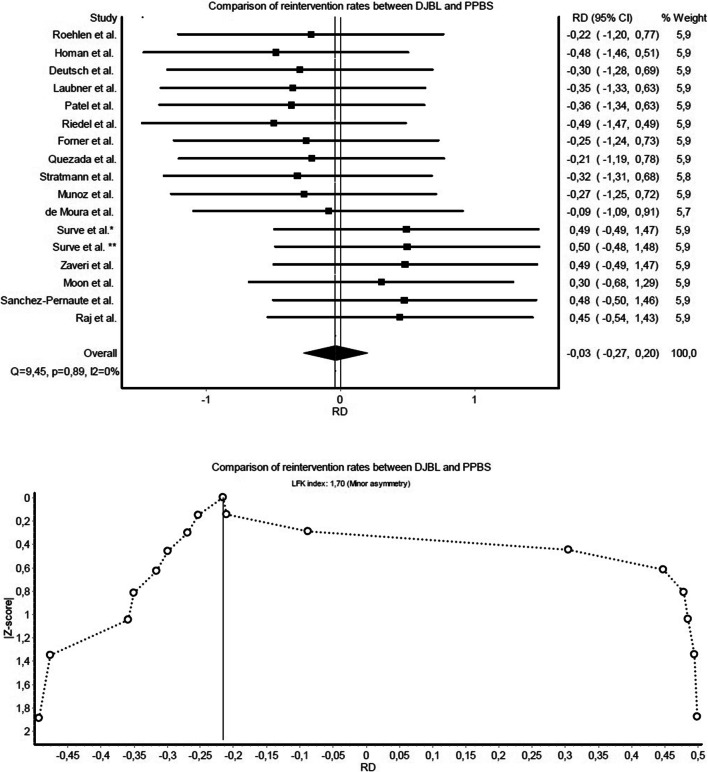
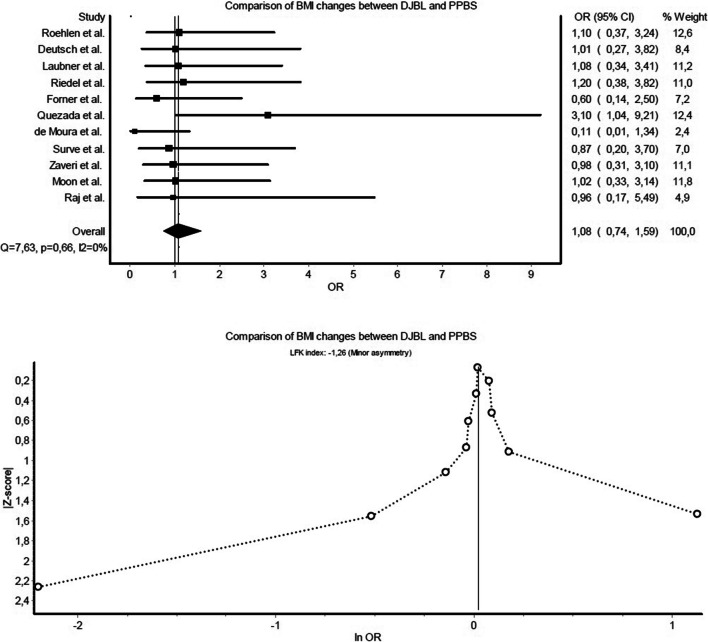
Results: A total of 11 publications on DJBL and 6 publications on PPBS were included, involving 800 and 1462 patients, respectively. The baseline characteristics of the patients were matched. Comparison of DJBL-related AEs and PPBS-related severe complications showed an almost equal risk (risk difference (RD): -0.03 and confidence interval (CI): -0.27 to 0.21), despite higher rates among patients having received endoscopic treatment. Overall AE and complication rates classified by Clavien-Dindo showed that PPBS was superior to DJBL due to an excess risk level of 25% (RD: 0.25, CI: 0.01-0.49). Reintervention rates were more favourable in the PPBS group, without significant differences in risk (RD: -0.03, CI: -0.27 to 0.20). However, PPBS seemed more efficient regarding weight loss outcomes at 1-year follow-up according to raw data, while meta-analysis did not reveal any significant difference (odds ratio (OR): 1.08, CI: 0.74-1.59 for BMI changes).
Conclusion: Only limited conclusions can be made based on our findings. PPBS was superior to DJBL with regard to safety outcomes (GRADE IIB), which failed to support the authors' hypothesis. Surgical procedures showed lower complication rates than the incidence of DJBL-related AEs, although it should be emphasized that the low number of PPBS-related mild to moderate complications reported could be the result of incomplete data recording from the analysed publications. Weight loss outcomes favoured bariatric surgery (GRADE IIB). As the DJBL is implanted into the upper gastrointestinal tract for 6 to 12 months, it seems a promising additional method in the inventory of metabolic interventions.
Keywords: Bariatric surgery; Duodenal switch; Duodeno-jejunal bypass liner; EndoBarrier; Metabolic surgery; Pylorus preserving; Single-anastomosis duodeno-ileal bypass; Single-anastomosis duodeno-jejunal bypass.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Aschner P. Recent advances in understanding/managing type 2 diabetes mellitus. F1000Res. 2017;6:pii: F1000 Faculty Rev-1922. doi: 10.12688/f1000research.11192.1. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
