

Cardiovascular Drug Therapy during Interstage After Hybrid Approach: A Single-Center Experience in 51 Newborns with Hypoplastic Left Heart
- PMID: 33713024
- PMCID: PMC7997825
- DOI: 10.1007/s40272-021-00438-2
Cardiovascular Drug Therapy during Interstage After Hybrid Approach: A Single-Center Experience in 51 Newborns with Hypoplastic Left Heart
Abstract
Background: Newborns with hypoplastic left heart (HLH) are usually palliated with the Norwood procedure or a hybrid stage I procedure. Hybrid is our preferred approach. Given the critical relationship between stage I, interstage, and comprehensive stage II or advanced biventricular repair, we hypothesized that appropriate drug treatment is a significant therapeutic cornerstone, especially for the management of the high-risk interstage.
Methods: We report a single-center observational study addressing the cardiovascular effects of, in particular, oral β-blockers and the additional use of angiotensin-converting enzyme (ACE) and mineralocorticoid inhibitors.
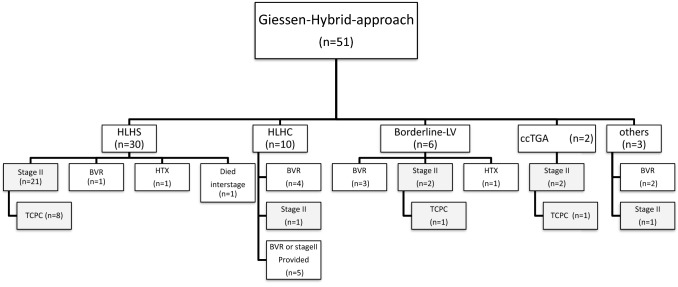
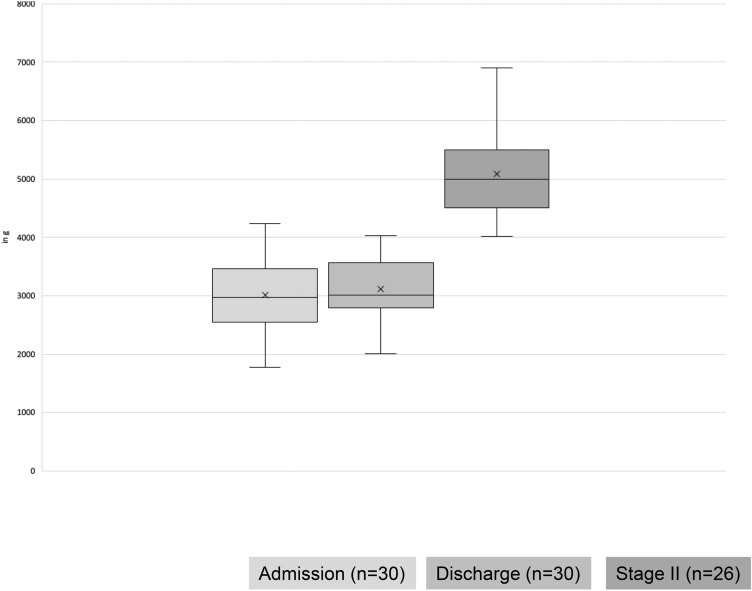
Results: In total, 51 newborns-30 with HLH syndrome (HLHS) and 21 with HLH complex (HLHC)-with a median bodyweight of 3.0 kg (range 1.9-4.4; nine with bodyweight ≤ 2500 g) underwent an uneventful "Giessen hybrid approach" using a newly approved duct stent. All patients were discharged home with a single, double or triple therapy consisting of ß-blockers, ACE and mineralocorticoid inhibitors; 90% of the patients received bisoprolol, 10% received propranolol, 72% received lisinopril, and 78% received spironolactone. Resting heart rate decreased from 138 bpm (range 112-172; n = 51) at admission to 123 bpm (range 99-139; n = 51) at discharge and 110 bpm before stage II/biventricular repair/heart transplantation (range 90-140; n = 37) accompanied by favorable bodyweight gain. No side effects were evident.
Conclusion: In view of drug risk/benefit profiles, as well as the variable morphology and hemodynamics, the highly selective β1-adrenoceptor blocker bisoprolol is our preferred drug for treatment of HLHS/HLHC in the interstage. We avoid using ACE inhibitor monotherapy and exclude potential risks for coronary and cerebral perfusion pressure beforehand.
Conflict of interest statement
Tino Mienert, Anoosh Esmaeili, Blanka Steinbrenner, Markus Khalil, Matthias Müller, Hakan Akintuerk, Gunter Kerst, and Dietmar Schranz have no conflicts of interest that are directly relevant to the content of this article.
Figures
Similar articles
-
Clinical course and interstage monitoring after the Norwood and hybrid procedures for hypoplastic left heart syndrome.Pediatr Cardiol. 2014 Jun;35(5):851-6. doi: 10.1007/s00246-014-0865-y. Epub 2014 Jan 18. Pediatr Cardiol. 2014. PMID: 24442219
-
Long-term results of biventricular repair after initial Giessen hybrid approach for hypoplastic left heart variants.J Thorac Cardiovasc Surg. 2015 Apr;149(4):1112-20; discussion 1120-2.e2. doi: 10.1016/j.jtcvs.2014.09.028. Epub 2014 Sep 18. J Thorac Cardiovasc Surg. 2015. PMID: 25439773
-
A Comprehensive Approach to the Management of Patients With HLHS and Related Malformations: An Analysis of 83 Patients (2015-2021).World J Pediatr Congenit Heart Surg. 2022 Sep;13(5):664-675. doi: 10.1177/21501351221088030. Epub 2022 May 5. World J Pediatr Congenit Heart Surg. 2022. PMID: 35511494 Review.
-
Interstage Survival for Patients with Hypoplastic Left Heart Syndrome After ECMO.Pediatr Cardiol. 2017 Jan;38(1):50-55. doi: 10.1007/s00246-016-1483-7. Epub 2016 Nov 1. Pediatr Cardiol. 2017. PMID: 27803957
-
Giessen Procedure as Comprehensive Stage II Palliation With Aortic Arch Reconstruction After Hybrid Bilateral Pulmonary Artery Banding and Ductal Stenting for Hypoplastic Left Heart Syndrome.Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2018 Mar;21:19-27. doi: 10.1053/j.pcsu.2017.11.007. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2018. PMID: 29425520 Review.
Cited by
-
Beta-blocker therapy in pediatric heart failure: 50 years lost to improve pharmacotherapy of a deadly disease.Ann Pediatr Cardiol. 2021 Jul-Sep;14(3):341-342. doi: 10.4103/apc.apc_126_21. Epub 2021 Aug 26. Ann Pediatr Cardiol. 2021. PMID: 34667405 Free PMC article. No abstract available.
-
A developmentally based proposal for neonates with hypoplastic left heart: What a great progress! But please don't stop here! A broad result is emerging.JTCVS Open. 2023 Sep 18;16:710-713. doi: 10.1016/j.xjon.2023.09.011. eCollection 2023 Dec. JTCVS Open. 2023. PMID: 38204644 Free PMC article. No abstract available.
-
Duct Stenting in Duct-Dependent Systemic Blood Flow, Past, Present, and Future.Pediatr Cardiol. 2025 Mar;46(3):515-524. doi: 10.1007/s00246-024-03492-y. Epub 2024 Apr 25. Pediatr Cardiol. 2025. PMID: 38664298 Free PMC article. Review.
-
Utility of the NEONATE Score at an Institution that Routinely Performs the Hybrid Procedure for Hypoplastic Left Heart Syndrome.Pediatr Cardiol. 2023 Dec;44(8):1684-1690. doi: 10.1007/s00246-023-03223-9. Epub 2023 Aug 26. Pediatr Cardiol. 2023. PMID: 37632588
References
-
- Michel-Behnke I, Akintuerk H, Marquardt I, Mueller M, Thul J, Bauer J, Hagel KJ, Kreuder J, Vogt P, Schranz D. Stenting of the ductus arteriosus and banding of the pulmonary arteries: basis for various surgical strategies in newborns with multiple left heart obstructive lesions. Heart. 2003;89(6):645–650. doi: 10.1136/heart.89.6.645. - DOI - PMC - PubMed
-
- Schranz D, Bauer A, Reich B, Steinbrenner B, Recla S, Schmidt D, Apitz C, Thul J, Valeske K, Bauer J, Müller M, Jux C, Michel-Behnke I, Akintürk H. Fifteen-year single center experience with the “Giessen Hybrid” approach for hypoplastic left heart and variants: current strategies and outcomes. Pediatr Cardiol. 2015;36(2):365–373. doi: 10.1007/s00246-014-1015-2. - DOI - PMC - PubMed
-
- Yerebakan C, Murray J, Valeske K, Thul J, Elmontaser H, Mueller M, Mann V, Ostermayer S, Latus H, Apitz C, Schranz D. Akintuerk H (2014) Long-term results of biventricular repair after initial Giessen hybrid approach for hypoplastic left heart variants. J Thorac Cardiovasc Surg. 2015;149:1112–1120. doi: 10.1016/j.jtcvs.2014.09.028. - DOI - PubMed
-
- Yerebakan C, Valeske K, Elmontaser H, Yörüker U, Mueller M, Thul J, Mann V, Latus H, Villanueva A, Hofmann K, Schranz D. Akintuerk H (2015) Hybrid therapy for hypoplastic left heart syndrome: myth, alternative, or standard? J Thorac Cardiovasc Surg. 2016;151:1112–1121. doi: 10.1016/j.jtcvs.2015.10.066. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
