

Improved coronary calcification quantification using photon-counting-detector CT: an ex vivo study in cadaveric specimens
- PMID: 33713174
- PMCID: PMC8380662
- DOI: 10.1007/s00330-021-07780-6
Improved coronary calcification quantification using photon-counting-detector CT: an ex vivo study in cadaveric specimens
Abstract
Objectives: To compare the accuracy of coronary calcium quantification of cadaveric specimens imaged from a photon-counting detector (PCD)-CT and an energy-integrating detector (EID)-CT.
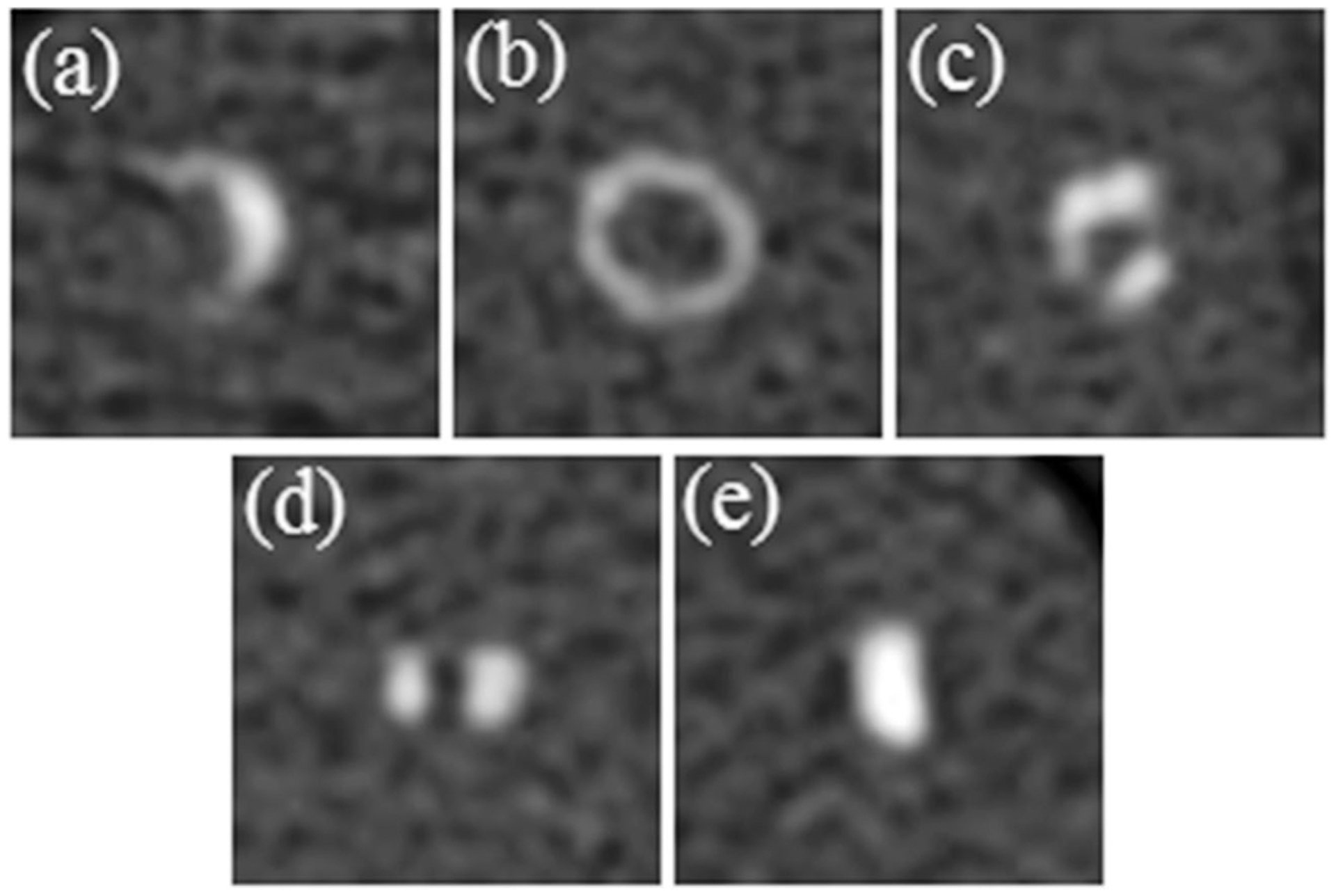
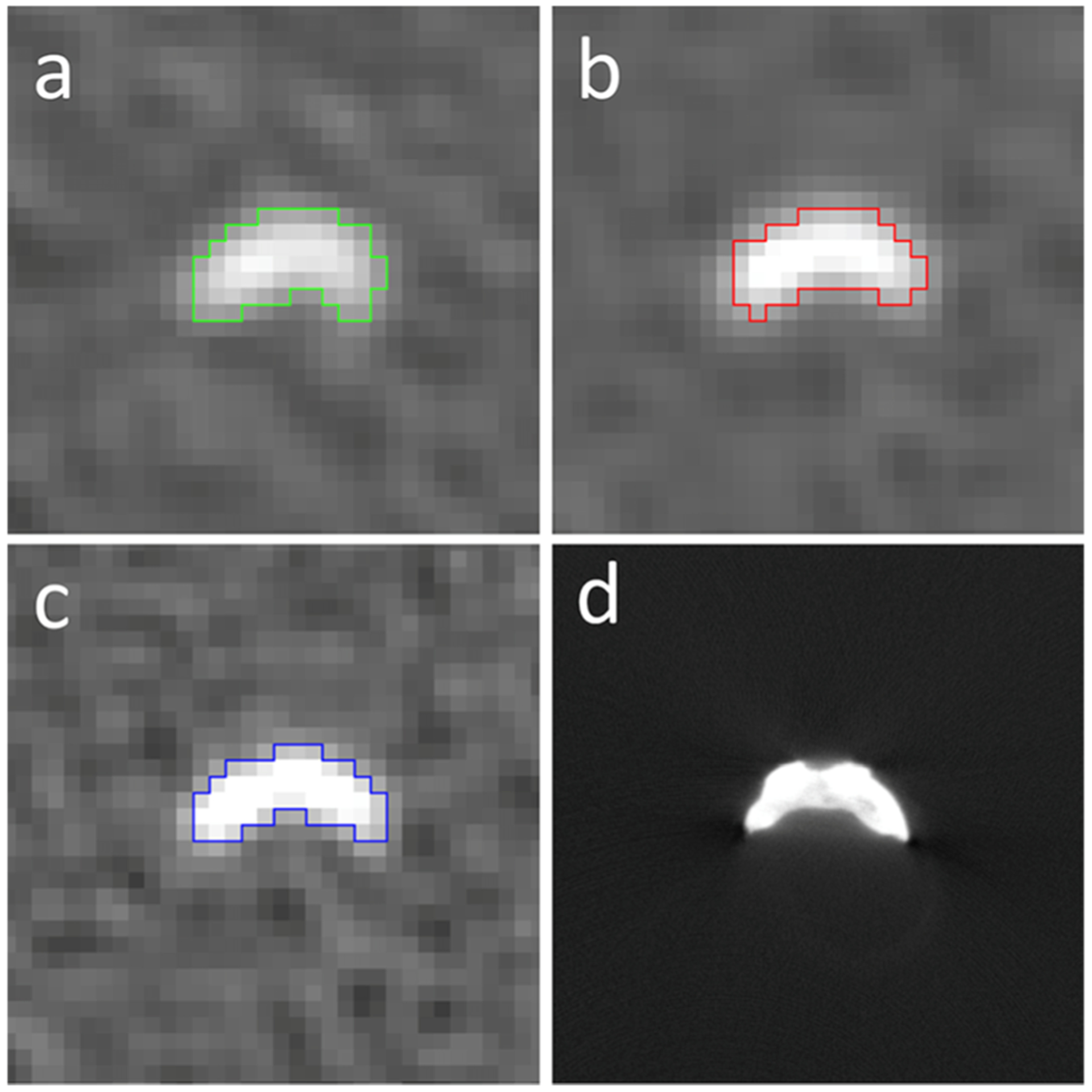
Methods: Excised coronary specimens were scanned on a PCD-CT scanner, using both the PCD and EID subsystems. The scanning and reconstruction parameters for EID-CT and PCD-CT were matched: 120 kV, 9.3-9.4 mGy CTDIvol, and a quantitative kernel (D50). PCD-CT images were also reconstructed using a sharper kernel (D60). Scanning the same specimens using micro-CT served as a reference standard for calcified volumes. Calcifications were segmented with a half-maximum thresholding technique. Segmented calcified volume differences were analyzed using the Friedman test and post hoc pairwise Wilcoxon signed rank test with the Bonferroni correction. Image noise measurements were compared between EID-CT and PCD-CT with a repeated-measures ANOVA test and post hoc pairwise comparison with the Bonferroni correction. A p < 0.05 was considered statistically significant.
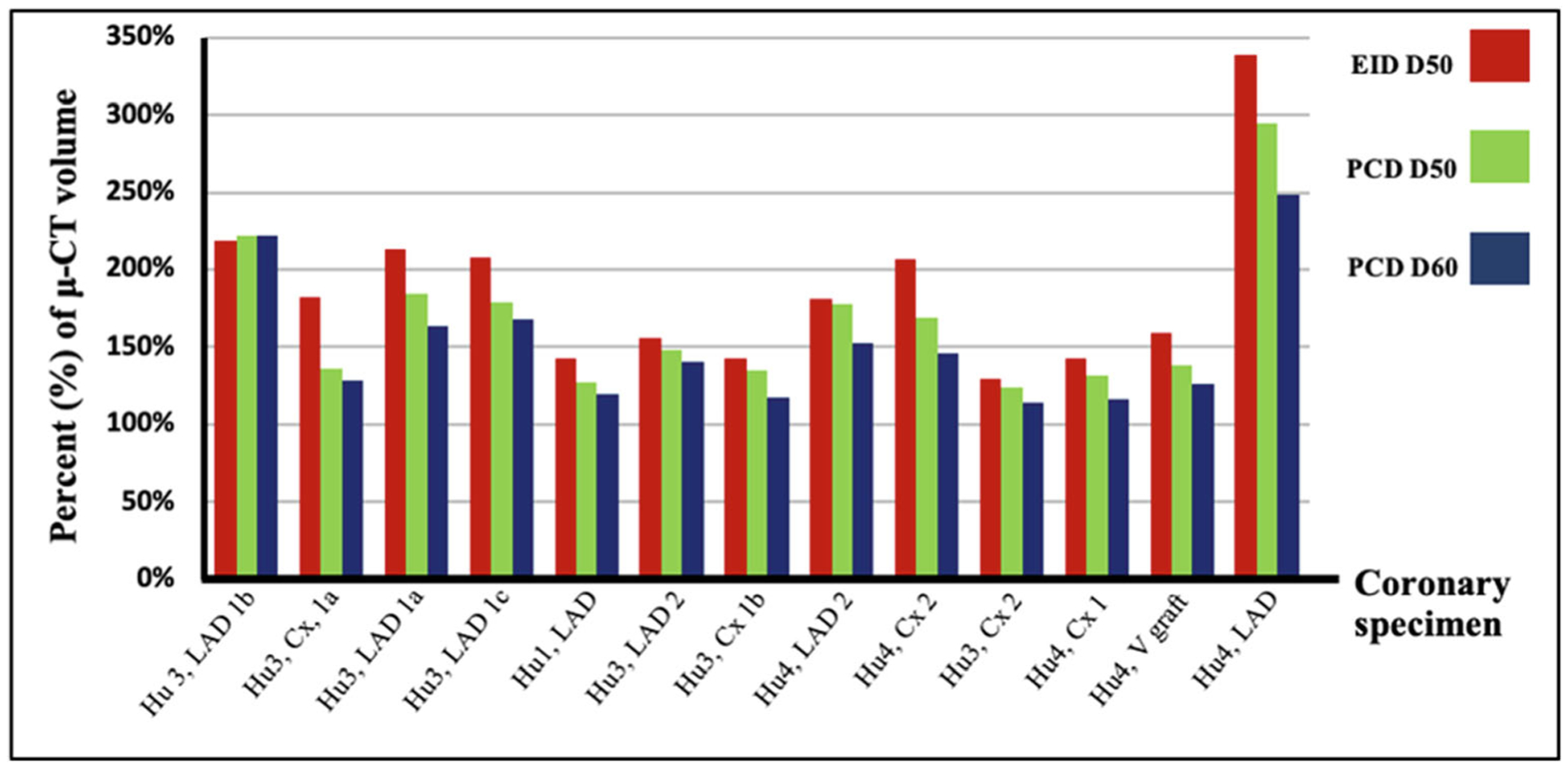
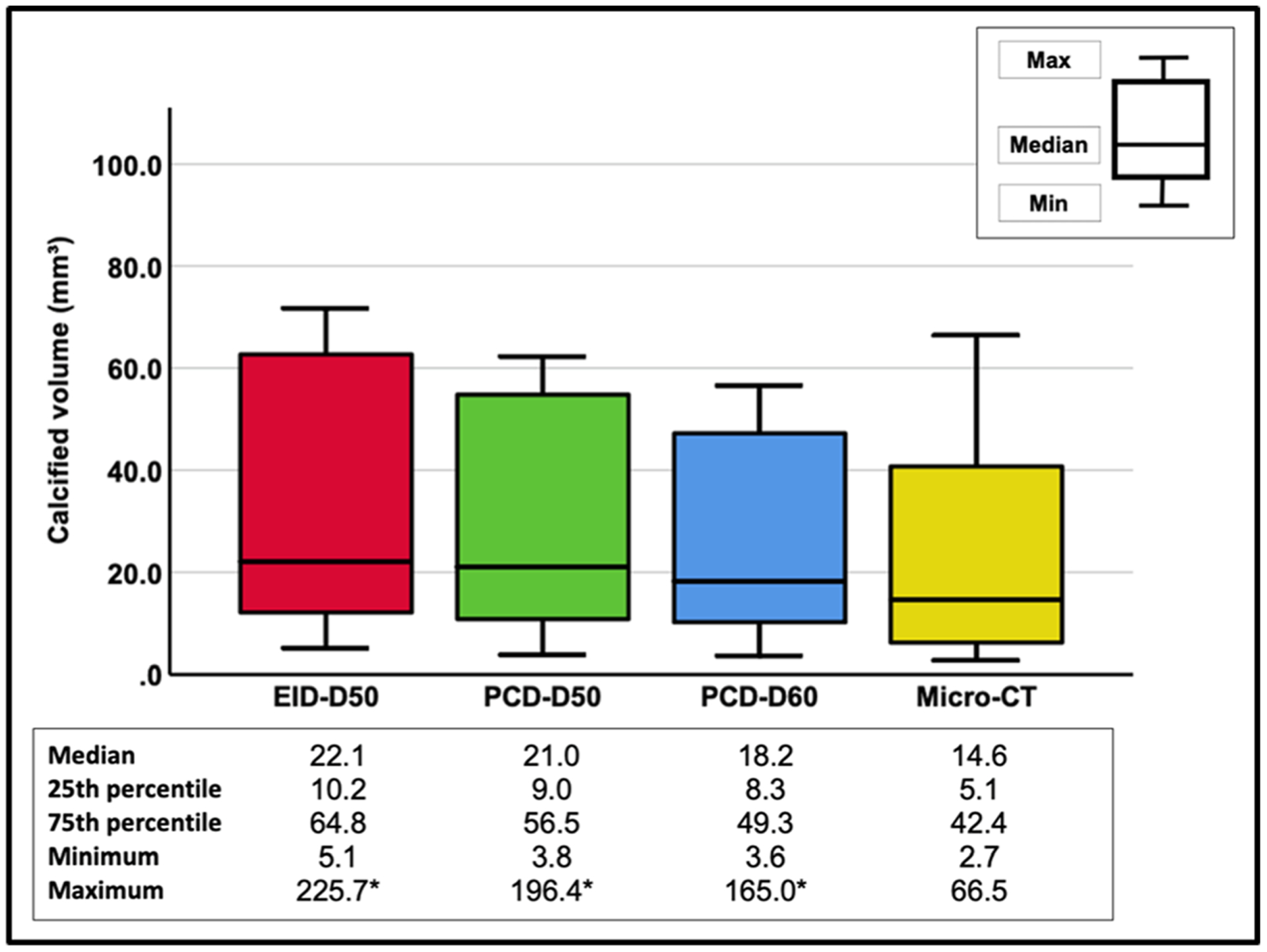
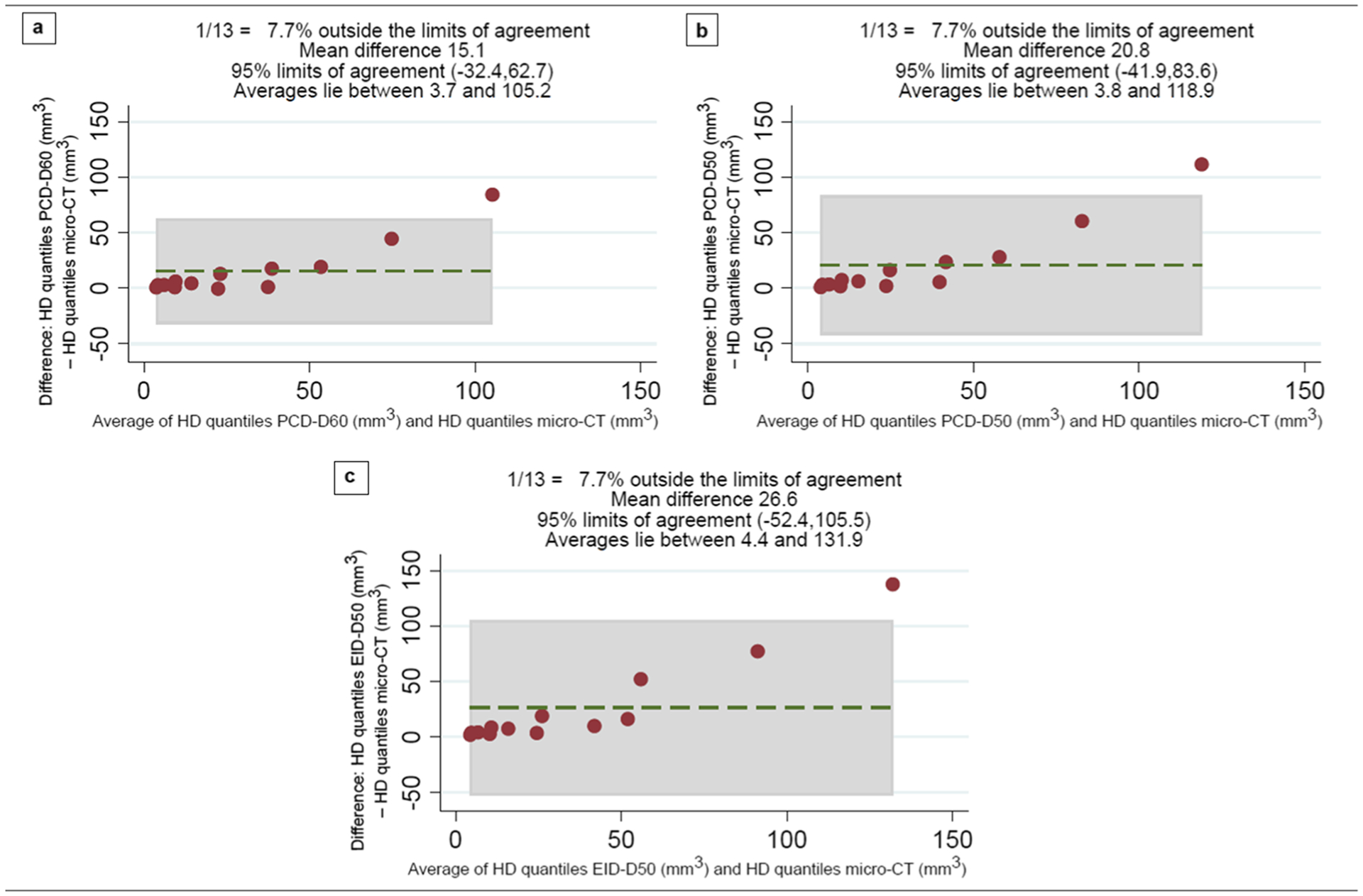
Results: The volume measurements in 12/13 calcifications followed a similar trend: EID-D50 > PCD-D50 > PCD-D60 > micro-CT. The median calcified volumes in EID-D50, PCD-D50, PCD-D60, and micro-CT were 22.1 (IQR 10.2-64.8), 21.0 (IQR 9.0-56.5), 18.2 (IQR 8.3-49.3), and 14.6 (IQR 5.1-42.4) mm3, respectively (p < 0.05 for all pairwise comparisons). The average image noise in EID-D50, PCD-D50, and PCD-D60 was 60.4 (± 3.5), 56.0 (± 4.2), and 113.6 (± 8.5) HU, respectively (p < 0.01 for all pairwise comparisons).
Conclusion: The PCT-CT system quantified coronary calcifications more accurately than EID-CT, and a sharp PCD-CT kernel further improved the accuracy. The PCD-CT images exhibited lower noise than the EID-CT images.
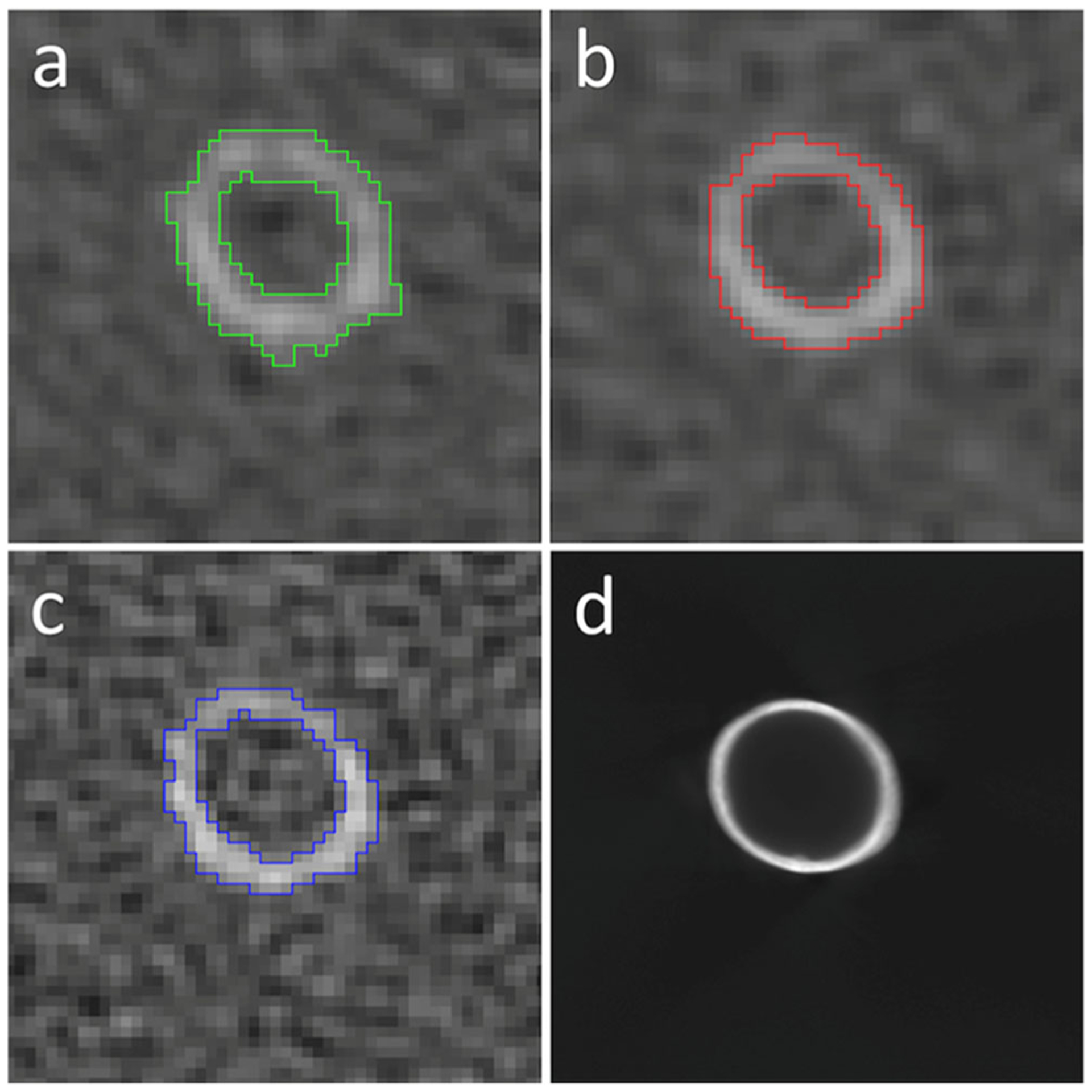
Key points: • High spatial resolution offered by PCD-CT reduces partial volume averaging and consequently leads to better morphological depiction of coronary calcifications. • Improved quantitative accuracy for coronary calcification volumes could be achieved using high-resolution PCD-CT compared to conventional EID-CT. • PCD-CT images exhibit lower image noise than conventional EID-CT at matched radiation dose and reconstruction kernel.
Keywords: Artifacts; Cadaver; Coronary artery disease; X-ray tomography.
© 2021. European Society of Radiology.
Figures
References
-
- Global Health Estimates (2016) Deaths by cause, age, sex, by country and by region, 2000–2016. World Health Organization, Geneva
-
- Sangiorgi G, Rumberger JA, Severson A et al. (1998) Arterial calcification and not lumen stenosis is highly correlated with atherosclerotic plaque burden in humans: a histologic study of 723 coronary artery segments using nondecalcifying methodology. J Am Coll Cardiol 31:126–133 - PubMed
-
- Rumberger JA, Simons DB, Fitzpatrick LA, Sheedy PF, Schwartz RS (1995) Coronary artery calcium area by electron-beam computed tomography and coronary atherosclerotic plaque area. A histopathologic correlative study. Circulation 92:2157–2162 - PubMed
-
- Detrano R, Guerci AD, Carr JJ et al. (2008) Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med 358:1336–1345 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
