

Community-based antibiotic access and use in six low-income and middle-income countries: a mixed-method approach
- PMID: 33713630
- PMCID: PMC8050200
- DOI: 10.1016/S2214-109X(21)00024-3
Community-based antibiotic access and use in six low-income and middle-income countries: a mixed-method approach
Abstract
Background: Antimicrobial misuse is common in low-income and middle-income countries (LMICs), and this practice is a driver of antibiotic resistance. We compared community-based antibiotic access and use practices across communities in LMICs to identify contextually specific targets for interventions to improve antibiotic use practices.
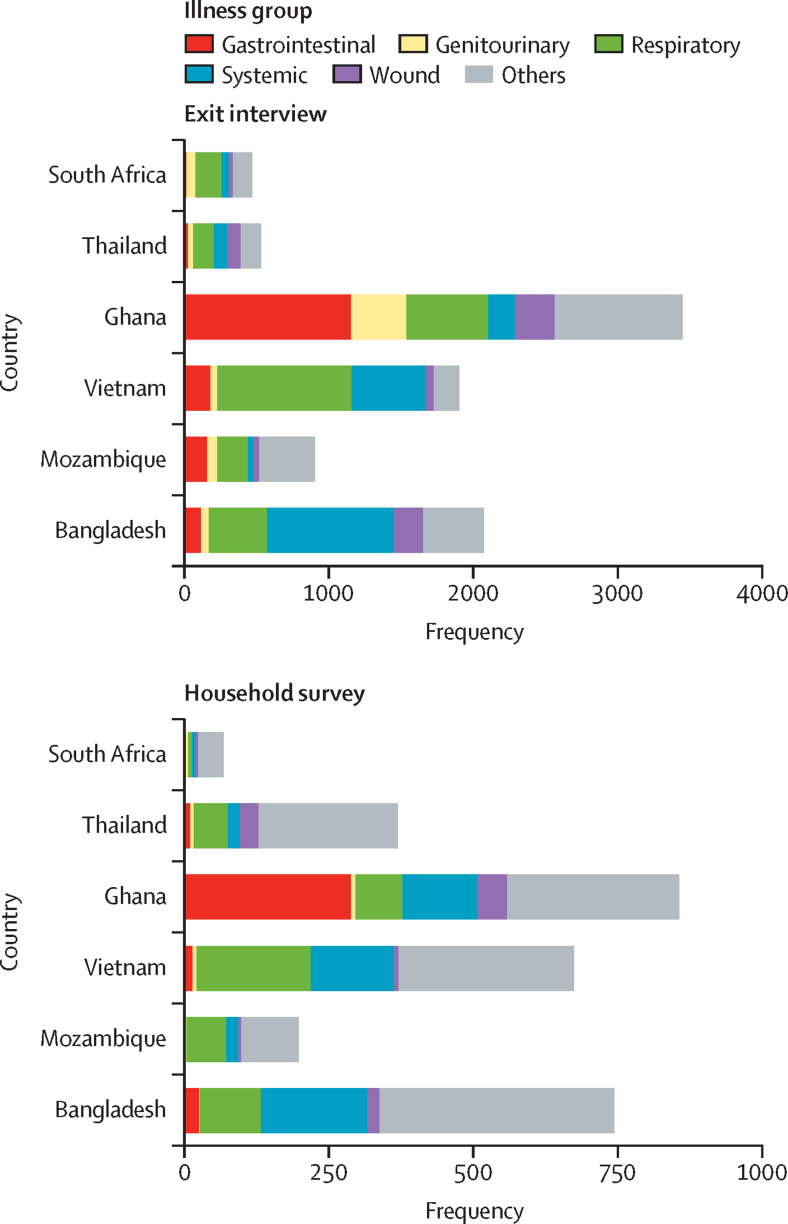
Methods: We did quantitative and qualitative assessments of antibiotic access and use in six LMICs across Africa (Mozambique, Ghana, and South Africa) and Asia (Bangladesh, Vietnam, and Thailand) over a 2·5-year study period (July 1, 2016-Dec 31, 2018). We did quantitative assessments of community antibiotic access and use through supplier mapping, customer exit interviews, and household surveys. These quantitative assessments were triangulated with qualitative drug supplier and consumer interviews and discussions.
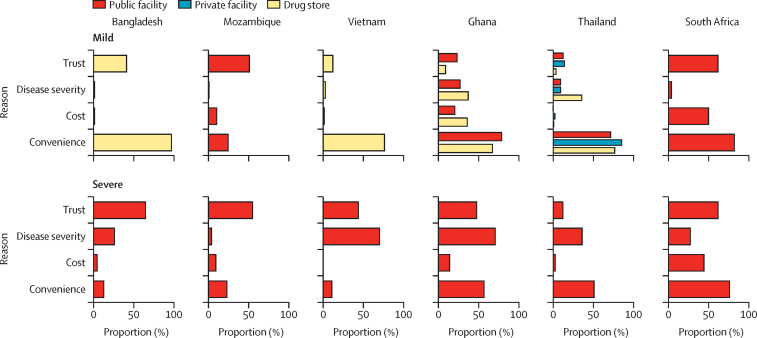
Findings: Vietnam and Bangladesh had the largest proportions of non-licensed antibiotic dispensing points. For mild illness, drug stores were the most common point of contact when seeking antibiotics in most countries, except South Africa and Mozambique, where public facilities were most common. Self-medication with antibiotics was found to be widespread in Vietnam (55·2% of antibiotics dispensed without prescription), Bangladesh (45·7%), and Ghana (36·1%), but less so in Mozambique (8·0%), South Africa (1·2%), and Thailand (3·9%). Self-medication was considered to be less time consuming, cheaper, and overall, more convenient than accessing them through health-care facilities. Factors determining where treatment was sought often involved relevant policies, trust in the supplier and the drug, disease severity, and whether the antibiotic was intended for a child. Confusion regarding how to identify oral antibiotics was revealed in both Africa and Asia.
Interpretation: Contextual complexities and differences between countries with different incomes, policy frameworks, and cultural norms were revealed. These contextual differences render a single strategy inadequate and instead necessitate context-tailored, integrated intervention packages to improve antibiotic use in LMICs as part of global efforts to combat antibiotic resistance.
Funding: Wellcome Trust and Volkswagen Foundation.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Access to antibiotics: not a problem in some LMICs.Lancet Glob Health. 2021 May;9(5):e561-e562. doi: 10.1016/S2214-109X(21)00085-1. Epub 2021 Mar 10. Lancet Glob Health. 2021. PMID: 33713631 No abstract available.
References
-
- Laxminarayan R, Duse A, Wattal C. Antibiotic resistance–the need for global solutions. Lancet Infect Dis. 2013;13:1057–1098. - PubMed
-
- Collignon P, Beggs JJ, Walsh TR, Gandra S, Laxminarayan R. Anthropological and socioeconomic factors contributing to global antimicrobial resistance: a univariate and multivariable analysis. Lancet Planet Health. 2018;2:e398–e405. - PubMed
-
- Fink G, D'Acremont V, Leslie HH, Cohen J. Antibiotic exposure among children younger than 5 years in low-income and middle-income countries: a cross-sectional study of nationally representative facility-based and household-based surveys. Lancet Infect Dis. 2020;20:179–187. - PubMed
-
- Van Boeckel TP, Gandra S, Ashok A. Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data. Lancet Infect Dis. 2014;14:742–750. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
