

Mitochondrial N-formyl methionine peptides associate with disease activity as well as contribute to neutrophil activation in patients with rheumatoid arthritis
- PMID: 33713887
- PMCID: PMC8062236
- DOI: 10.1016/j.jaut.2021.102630
Mitochondrial N-formyl methionine peptides associate with disease activity as well as contribute to neutrophil activation in patients with rheumatoid arthritis
Abstract
Objectives: Literature suggests that neutrophils of patients with rheumatoid arthritis (RA) are primed to respond to N-formyl methionine group (formylated peptides). Animal models indicate that formylated peptides contribute to joint damage via neutrophil recruitment and inflammation in joints. Non-steroidal anti-inflammatory drugs are also known to inhibit formyl peptide-induced neutrophil activation. The predominant source of formylated peptides in sterile inflammatory conditions like RA is mitochondria, organelles with prokaryotic molecular signatures. However, there is no direct evidence of mitochondrial formyl peptides (mtNFPs) in the circulation of patients with RA and their potential role in neutrophil-mediated inflammation in RA, including their clinical significance.
Methods: Levels of mtNFPs (total fMet, MT-ND6) were analyzed using ELISA in plasma and serum obtained from patients in 3 cross-sectional RA cohorts (n = 275), a longitudinal inception cohort (n = 192) followed for a median of 8 years, and age/gender-matched healthy controls (total n = 134). Neutrophil activation assays were done in the absence or presence of formyl peptide receptor 1 (FPR1) inhibitor cyclosporine H.
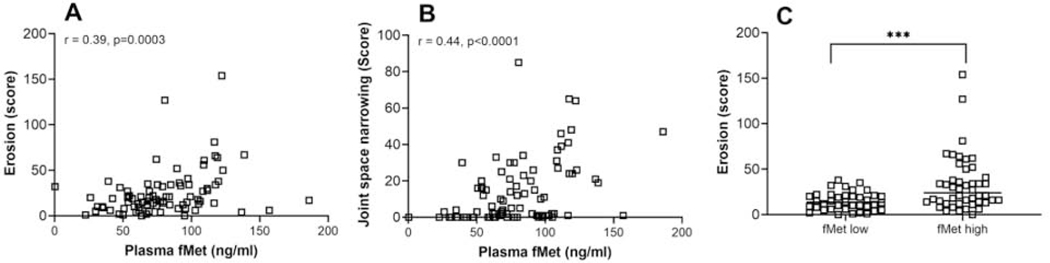
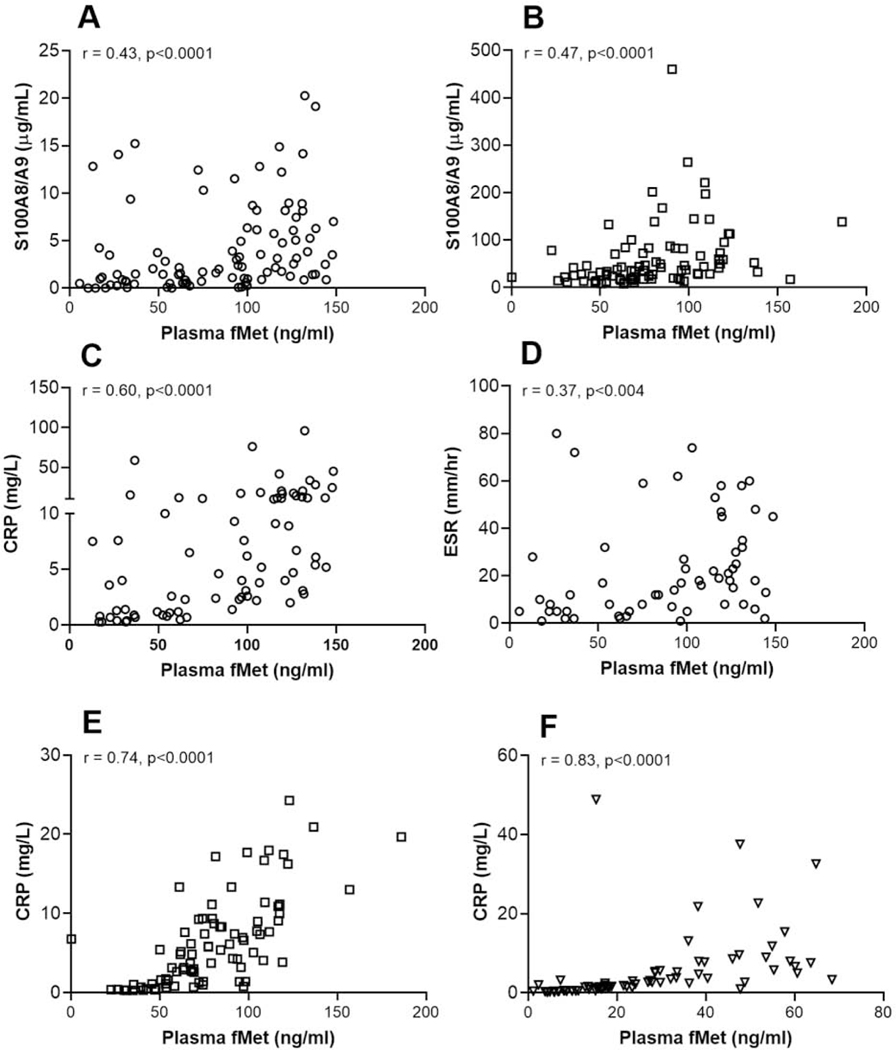
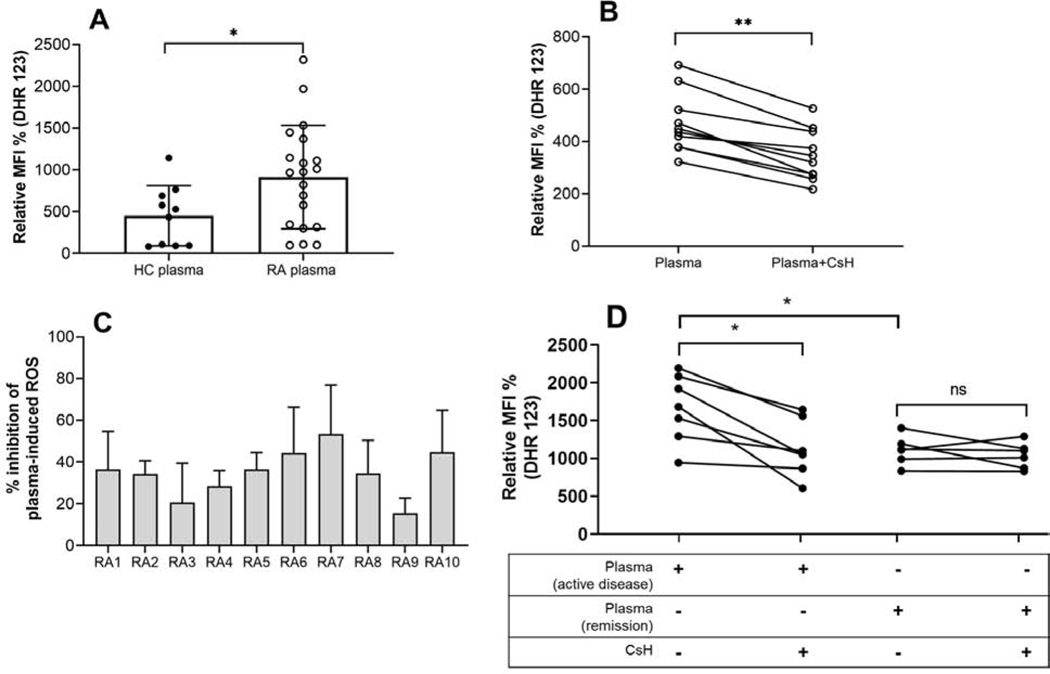
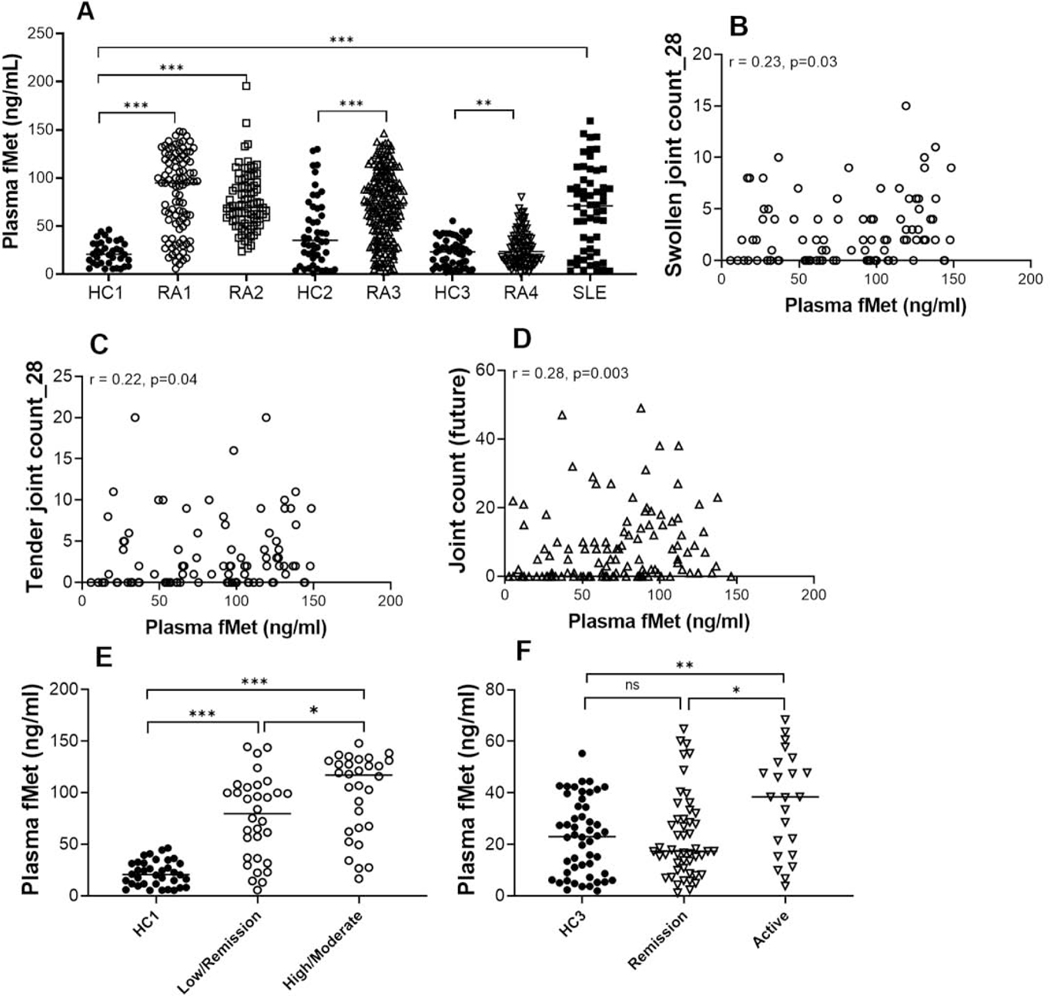
Results: Elevated levels of total fMet were observed in the circulation of patients with RA as compared to healthy controls (p < 0.0001) associating with disease activity and could distinguish patients with the active disease from patients with inactive disease or patients in remission. Baseline levels of total fMet correlated with current and future joint involvement, respectively and predicted the development of rheumatoid nodules (OR = 1.2, p = 0.04). Further, total fMet levels improved the prognostic ability of ACPA in predicting erosive disease (OR of 7.9, p = 0.001). Total fMet levels correlated with markers of inflammation and neutrophil activation. Circulating mtNFPs induced neutrophil activation in vitro through FPR1-dependent mechanisms.
Conclusions: Circulating mtNFPs could be novel biomarkers of disease monitoring and prognosis for RA and in investigating neutrophil-mediated inflammation in RA. We propose, FPR1 as a novel therapeutic target for RA.
Keywords: Clinical biomarkers; Formyl peptide receptor 1; Mitochondria; Neutrophils; Rheumatoid arthritis.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Figures
References
-
- McInnes IB, Schett G. The pathogenesis of rheumatoid arthritis. N Engl J Med, 2011;365:2205–19. - PubMed
-
- Wipke BT, Allen PM. Essential role of neutrophils in the initiation and progression of a murine model of rheumatoid arthritis. J Immunol, 2001;167:1601–8. - PubMed
-
- Wright HL, Chikura B, Bucknall RC, Moots RJ, Edwards SW. Changes in expression of membrane TNF, NF-{kappa}B activation and neutrophil apoptosis during active and resolved inflammation. Ann Rheum Dis, 2011;70:537–43. - PubMed
-
- Mantovani A, Cassatella MA, Costantini C, Jaillon S. Neutrophils in the activation and regulation of innate and adaptive immunity. Nat Rev Immunol, 2011;11:519–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
