

Insulin resistance, diabetic kidney disease, and all-cause mortality in individuals with type 2 diabetes: a prospective cohort study
- PMID: 33715620
- PMCID: PMC7962330
- DOI: 10.1186/s12916-021-01936-3
Insulin resistance, diabetic kidney disease, and all-cause mortality in individuals with type 2 diabetes: a prospective cohort study
Abstract
Background: It is unclear whether insulin resistance (IR) contributes to excess mortality in patients with type 2 diabetes independent of diabetic kidney disease (DKD), which is strongly associated with IR and is a major risk factor for cardiovascular disease (CVD), the main cause of death in these individuals. We tested this hypothesis in patients with type 2 diabetes from the Renal Insufficiency And Cardiovascular Events Italian Multicentre Study.
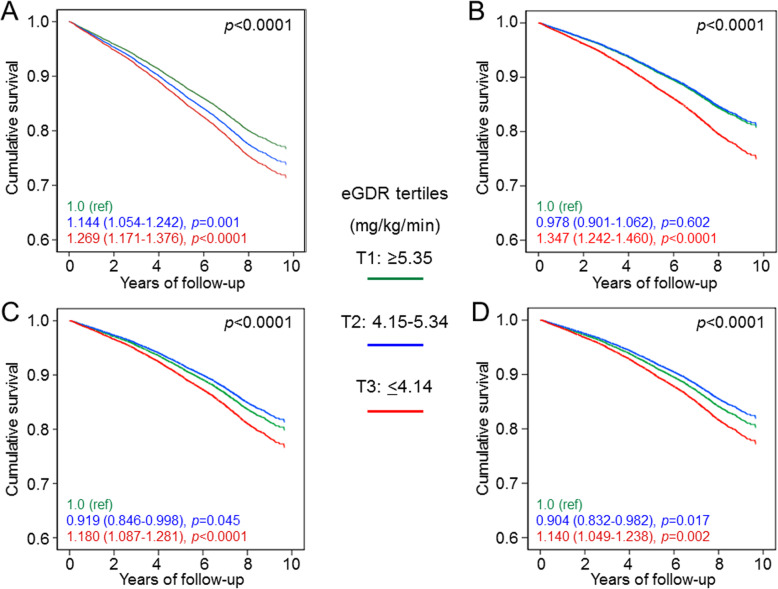
Methods: This observational, prospective, cohort study enrolled 15,773 patients with type 2 diabetes attending 19 Italian Diabetes Clinics in 2006-2008. Insulin sensitivity was assessed as estimated glucose disposal rate (eGDR), which was validated against the euglycaemic-hyperinsulinemic clamp technique. Vital status on October 31, 2015, was retrieved for 15,656 patients (99.3%). Participants were stratified by eGDR tertiles from T1 (≥ 5.35 mg/kg/min) to T3 (≤ 4.14 mg/kg/min, highest IR).
Results: CVD risk profile was worse in T2 and T3 vs T1. eGDR tertiles were independently associated with micro- and macroalbuminuria and the albuminuric DKD phenotypes (albuminuria with preserved or reduced estimated glomerular filtration rate [eGFR]) as well as with eGFR categories or the nonalbuminuric DKD phenotype. Over a 7.4-year follow-up, unadjusted death rates and mortality risks increased progressively across eGDR tertiles, but remained significantly elevated after adjustment only in T3 vs T1 (age- and gender- adjusted death rate, 22.35 vs 16.74 per 1000 person-years, p < 0.0001, and hazard ratio [HR] adjusted for multiple confounders including DKD, 1.140 [95% confidence interval [CI], 1.049-1.238], p = 0.002). However, eGDR was independently associated with mortality in participants with no DKD (adjusted HR, 1.214 [95% CI, 1.072-1.375], p = 0.002) and in those with nonalbuminuric DKD (1.276 [1.034-1.575], p = 0.023), but not in those with the albuminuric DKD phenotypes. Moreover, the association was stronger in males and in younger individuals and was observed in those without but not with prior CVD, though interaction was significant only for age.
Conclusions: The proxy of insulin sensitivity eGDR predicts all-cause mortality in type 2 diabetes, independent of confounders including DKD. However, the impact of IR in individuals with albuminuric DKD may be mediated by its relationship with albuminuria.
Trial registration: ClinicalTrials.gov , NCT00715481, retrospectively registered 15 July 2008.
Keywords: Albuminuria; All-cause mortality; Diabetic kidney disease; Estimated glucose disposal rate; Glomerular filtration rate; Mellitus; Type 2 diabetes.
Conflict of interest statement
G.Pe.: lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novo Nordisk, Sigma-Tau, and Takeda, and travel grants from AstraZeneca, Novo Nordisk, and Takeda; A.S.: consulting fees from AstraZeneca, Boehringer Ingelheim, and Sanofi-Aventis, and lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, and MundiPharma; E.O.: consulting fees from Eli Lilly and Novo Nordisk; E.B.: consulting fees from Abbot, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Bruno Farmaceutici, Eli Lilly, Janssen, Johnson&Johnson, Merck Sharp & Dohme, MundiPharma, Novartis, Novo Nordisk, Roche, Sanofi-Aventis, Servier, and Takeda, and research grants from AstraZeneca, Genzyme, Menarini Diagnostics, Novo Nordisk, Roche, and Takeda; C.F.: lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, and Novo Nordisk and travel grants from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Sanofi-Aventis, and Takeda; R.T.: consulting fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novo Nordisk, and Sanofi-Aventis, and lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, and Novo Nordisk; M.V.: lecture fees from Lifescan and Novo Nordisk; F.C.: lecture fees from AstraZeneca, Sanofi-Aventis, and Takeda; G.Z.: research grants from NTC Pharma and Omikron Italia; O.L.: consulting fees from Astra-Zeneca, Boehringer Ingelheim; lecture fees from Astra-Zeneca, Eli-Lilly, Merck-Sharp&Dohme, Sigma-Tau, Sanofi-Aventis, Takeda; grant support from Astra-Zeneca; A.N.: consulting fees from AstraZeneca, Pikdare, and Roche, lecture fees from AstraZeneca, Boehringer Ingelheim, Medtronic, and Novo Nordisk, and research grants from Aboca, AstraZeneca, Eli Lilly, Novo Nordisk, Sanofi-Aventis, and Theras; G.Pu.: consulting fees from AstraZeneca, Boehringer Ingelheim, and Eli Lilly, lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, MundiPharma, Novartis, Novo Nordisk, Sigma-Tau, Takeda, and travel grants from AstraZeneca, Laboratori Guidotti, Sanofi-Aventis, and Takeda.
Figures

References
-
- Penno G, Solini A, Bonora E, Orsi E, Fondelli C, Zerbini G, et al. Defining the contribution of chronic kidney disease to all-cause mortality in patients with type 2 diabetes: the Renal Insufficiency And Cardiovascular Events (RIACE) Italian Multicenter Study. Acta Diabetol. 2018;55:603–612. doi: 10.1007/s00592-018-1133-z. - DOI - PubMed
-
- Gregg EW, Cheng YJ, Srinivasan M, Lin J, Geiss LS, Albright AL, et al. Trends in cause-specific mortality among adults with and without diagnosed diabetes in the USA: an epidemiological analysis of linked national survey and vital statistics data. Lancet. 2018;391:2430–2440. doi: 10.1016/S0140-6736(18)30314-3. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
