

Fine Tuning of Traumatic Brain Injury Management in Neurointensive Care-Indicative Observations and Future Perspectives
- PMID: 33716941
- PMCID: PMC7943830
- DOI: 10.3389/fneur.2021.638132
Fine Tuning of Traumatic Brain Injury Management in Neurointensive Care-Indicative Observations and Future Perspectives
Abstract
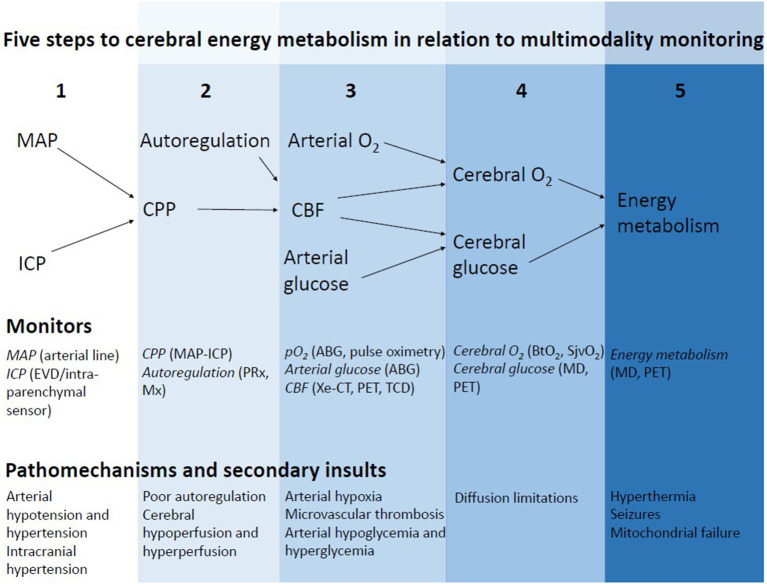
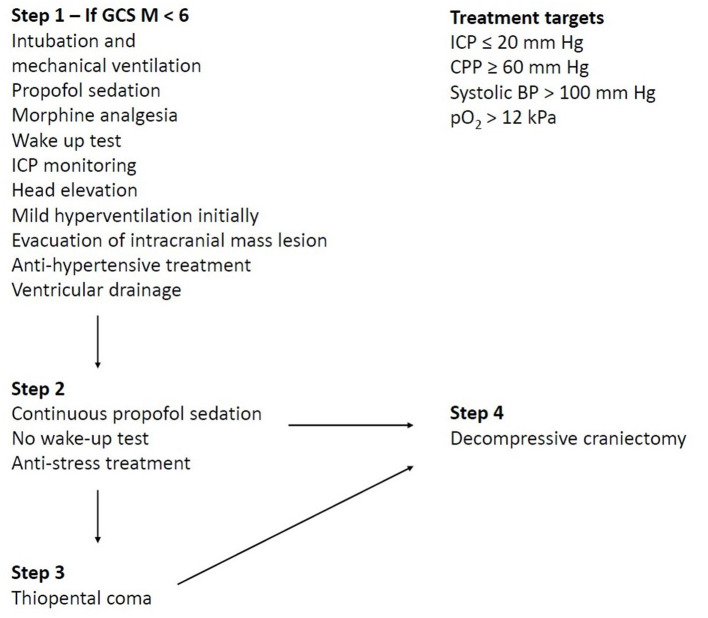
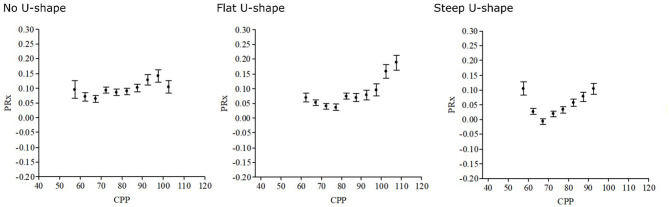
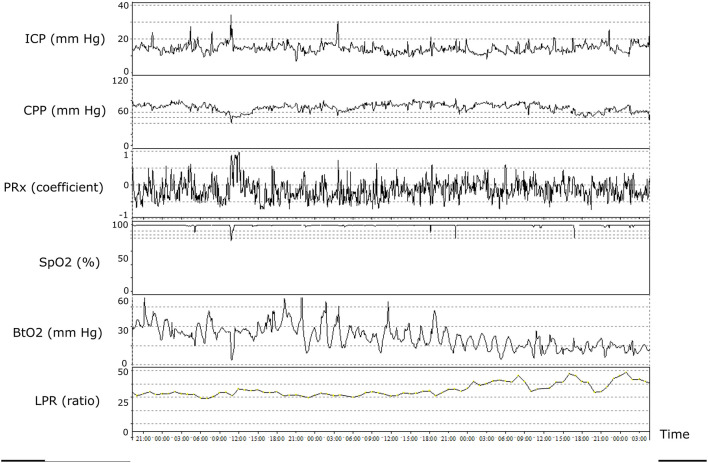
Neurointensive care (NIC) has contributed to great improvements in clinical outcomes for patients with severe traumatic brain injury (TBI) by preventing, detecting, and treating secondary insults and thereby reducing secondary brain injury. Traditional NIC management has mainly focused on generally applicable escalated treatment protocols to avoid high intracranial pressure (ICP) and to keep the cerebral perfusion pressure (CPP) at sufficiently high levels. However, TBI is a very heterogeneous disease regarding the type of injury, age, comorbidity, secondary injury mechanisms, etc. In recent years, the introduction of multimodality monitoring, including, e.g., pressure autoregulation, brain tissue oxygenation, and cerebral energy metabolism, in addition to ICP and CPP, has increased the understanding of the complex pathophysiology and the physiological effects of treatments in this condition. In this article, we will present some potential future approaches for more individualized patient management and fine-tuning of NIC, taking advantage of multimodal monitoring to further improve outcome after severe TBI.
Keywords: multimodality monitoring; neurointensive care; secondary brain injury; secondary insults; traumatic brain injury.
Copyright © 2021 Svedung Wettervik, Lewén and Enblad.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Fine tuning of neurointensive care in aneurysmal subarachnoid hemorrhage: From one-size-fits-all towards individualized care.World Neurosurg X. 2023 Jan 24;18:100160. doi: 10.1016/j.wnsx.2023.100160. eCollection 2023 Apr. World Neurosurg X. 2023. PMID: 36818739 Free PMC article. Review.
-
Introduction of the Uppsala Traumatic Brain Injury register for regular surveillance of patient characteristics and neurointensive care management including secondary insult quantification and clinical outcome.Ups J Med Sci. 2013 Aug;118(3):169-80. doi: 10.3109/03009734.2013.806616. Ups J Med Sci. 2013. PMID: 23837596 Free PMC article.
-
Neurointensive care of traumatic brain injury in the elderly-age-specific secondary insult levels and optimal physiological levels to target need to be defined.Acta Neurochir (Wien). 2022 Jan;164(1):117-128. doi: 10.1007/s00701-021-05047-z. Epub 2021 Nov 10. Acta Neurochir (Wien). 2022. PMID: 34757477 Free PMC article.
-
Temporal Neurophysiological Dynamics in Traumatic Brain Injury: Role of Pressure Reactivity and Optimal Cerebral Perfusion Pressure for Predicting Outcome.J Neurotrauma. 2019 Jun;36(11):1818-1827. doi: 10.1089/neu.2018.6157. Epub 2019 Feb 25. J Neurotrauma. 2019. PMID: 30595128
-
Intracranial pressure monitoring, cerebral perfusion pressure estimation, and ICP/CPP-guided therapy: a standard of care or optional extra after brain injury?Br J Anaesth. 2014 Jan;112(1):35-46. doi: 10.1093/bja/aet418. Epub 2013 Nov 28. Br J Anaesth. 2014. PMID: 24293327 Review.
Cited by
-
Traumatic brain injury causes early aggregation of beta-amyloid peptides and NOTCH3 reduction in vascular smooth muscle cells of leptomeningeal arteries.Acta Neuropathol. 2025 Jan 22;149(1):10. doi: 10.1007/s00401-025-02848-9. Acta Neuropathol. 2025. PMID: 39841284 Free PMC article.
-
Red solid line: Patterns of terminal loss of cerebrovascular reactivity at the bedside.Brain Spine. 2024 Jan 27;4:102760. doi: 10.1016/j.bas.2024.102760. eCollection 2024. Brain Spine. 2024. PMID: 38510604 Free PMC article.
-
Association of Arterial Metabolic Content with Cerebral Blood Flow Regulation and Cerebral Energy Metabolism-A Multimodality Analysis in Aneurysmal Subarachnoid Hemorrhage.J Intensive Care Med. 2022 Nov;37(11):1442-1450. doi: 10.1177/08850666221080054. Epub 2022 Feb 16. J Intensive Care Med. 2022. PMID: 35171061 Free PMC article.
-
ICP, PRx, CPP, and ∆CPPopt in pediatric traumatic brain injury: the combined effect of insult intensity and duration on outcome.Childs Nerv Syst. 2023 Sep;39(9):2459-2466. doi: 10.1007/s00381-023-05982-5. Epub 2023 Jun 3. Childs Nerv Syst. 2023. PMID: 37270434 Free PMC article.
-
Fine tuning of neurointensive care in aneurysmal subarachnoid hemorrhage: From one-size-fits-all towards individualized care.World Neurosurg X. 2023 Jan 24;18:100160. doi: 10.1016/j.wnsx.2023.100160. eCollection 2023 Apr. World Neurosurg X. 2023. PMID: 36818739 Free PMC article. Review.
References
-
- Guillaume J, Janny P. Continuous intracranial manometry; physiopathologic and clinical significance of the method. La Presse medicale. (1951) 59:953–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources