

Familial Hyperparathyroidism
- PMID: 33716975
- PMCID: PMC7947864
- DOI: 10.3389/fendo.2021.623667
Familial Hyperparathyroidism
Abstract
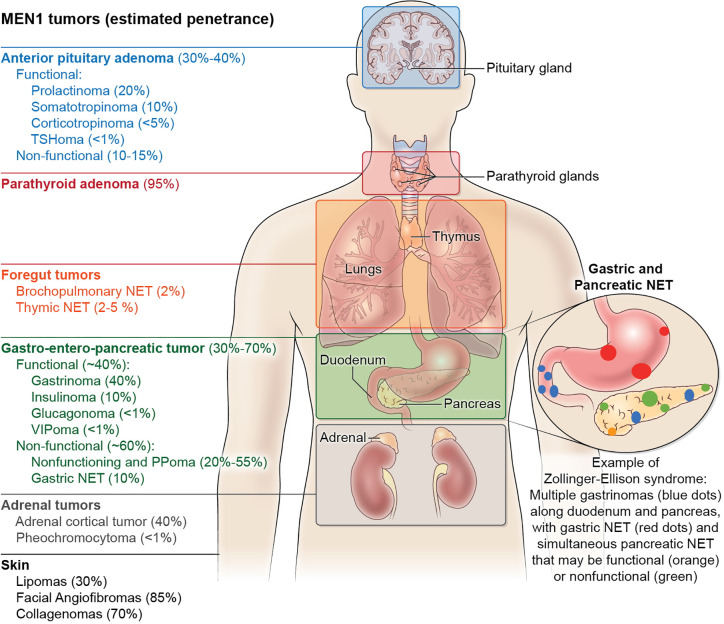
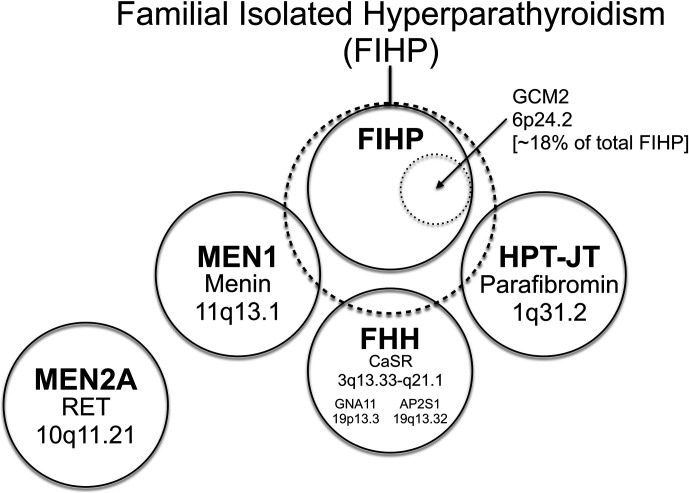
Regulation of the serum calcium level in humans is achieved by the endocrine action of parathyroid glands working in concert with vitamin D and a set of critical target cells and tissues including osteoblasts, osteoclasts, the renal tubules, and the small intestine. The parathyroid glands, small highly vascularized endocrine organs located behind the thyroid gland, secrete parathyroid hormone (PTH) into the systemic circulation as is needed to keep the serum free calcium concentration within a tight physiologic range. Primary hyperparathyroidism (HPT), a disorder of mineral metabolism usually associated with abnormally elevated serum calcium, results from the uncontrolled release of PTH from one or several abnormal parathyroid glands. Although in the vast majority of cases HPT is a sporadic disease, it can also present as a manifestation of a familial syndrome. Many benign and malignant sporadic parathyroid neoplasms are caused by loss-of-function mutations in tumor suppressor genes that were initially identified by the study of genomic DNA from patients who developed HPT as a manifestation of an inherited syndrome. Somatic and inherited mutations in certain proto-oncogenes can also result in the development of parathyroid tumors. The clinical and genetic investigation of familial HPT in kindreds found to lack germline variants in the already known HPT-predisposition genes represents a promising future direction for the discovery of novel genes relevant to parathyroid tumor development.
Keywords: CASR; CDC73; GCM2; MEN1; jaw tumor syndrome; multiple endocrine neoplasia; oncogene; tumor suppressor.
Copyright © 2021 Blau and Simonds.
Conflict of interest statement
JB is employed by the company AstraZeneca. The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The handling editor declared a past co-authorship with the authors JB and WS.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources