

Coagulation disorders and thromboembolic disease in COVID-19: review of current evidence in search of a better approach
- PMID: 33717596
- PMCID: PMC7947499
- DOI: 10.21037/jtd-20-3062
Coagulation disorders and thromboembolic disease in COVID-19: review of current evidence in search of a better approach
Abstract
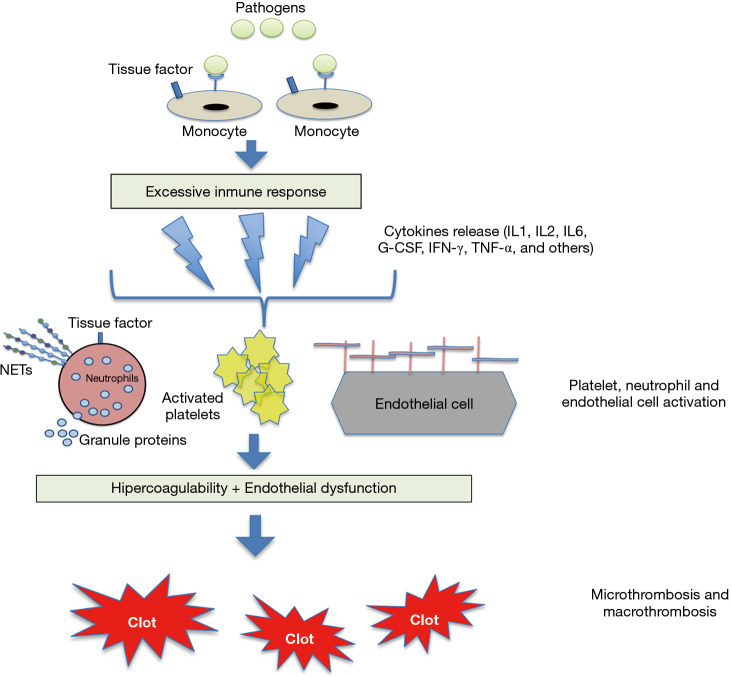
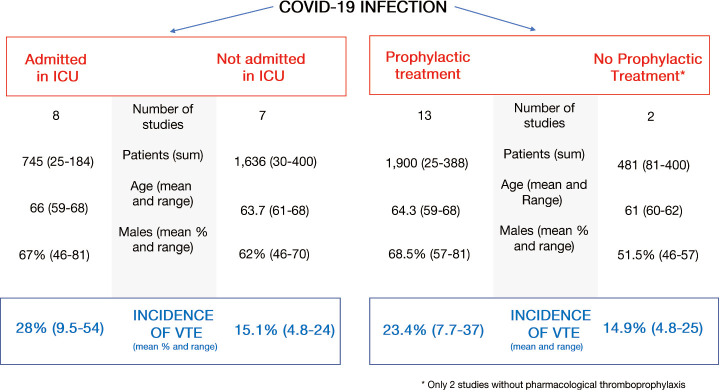
The new severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has been an unprecedented global health problem, causing more than 20 million infections and more than 900,000 deaths (September 2020). The SARS-CoV-2 infection, known as COVID-19, has various clinical presentations, from asymptomatic or mild catarrhal processes to severe pneumonia that rapidly progresses to acute respiratory distress syndrome (ARDS) and multiple organ failure. In the last few months, much scientific literature has been devoted to descriptions of different aspects of the coagulation disorders and arterial and venous thrombotic complications associated with COVID-19, particularly venous thromboembolism (VTE). These studies have revealed that SARS-CoV-2 could lead to a prothrombotic state reflecting the high cumulative incidence of associated thrombotic events, particularly in patients admitted to intensive care units (ICUs). As regards the coagulopathy observed in association with SARS-CoV-2 infection, the mechanisms that activate coagulation have been hypothesized as being linked to immune responses, through the release of pro-inflammatory mediators that interact with platelets, stimulate the expression of tissue factor, induce an upregulation of plasminogen activator inhibitor-1, suppress the fibrinolytic system and lead to endothelial dysfunction, triggering thrombogenesis. D-dimer elevation has been recognized as a useful biomarker of poor prognosis, although the best cut-off point for predicting VTE in COVID-19 patients has still not been clarified. This review will try to update all the available scientific information on this important topic with enormous clinical and therapeutic implications.
Keywords: D-dimer; Pulmonary embolism (PE); coronavirus disease 2019 (COVID-19); inflammation; thrombosis.
2021 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jtd-20-3062). All authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous