

Analysis of vertical and horizontal offsets in displaced femoral neck fracture in elderly treated with indigenous bicentric bipolar hip device
- PMID: 33717886
- PMCID: PMC7920007
- DOI: 10.1016/j.jcot.2020.11.014
Analysis of vertical and horizontal offsets in displaced femoral neck fracture in elderly treated with indigenous bicentric bipolar hip device
Abstract
Objectives: To analyze the effect of indigenous bicentric bipolar prosthesis on horizontal and vertical offsets in fracture neck of femur when compared to contralateral normal hip and to evaluate functional outcomes. We hypothesized that our non-modular bipolar device restores satisfactory offsets in such patients.
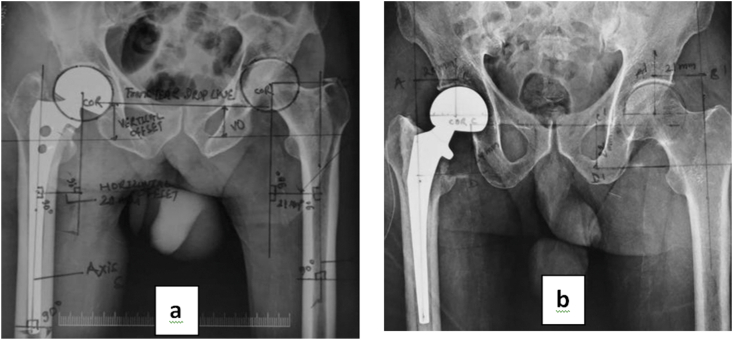
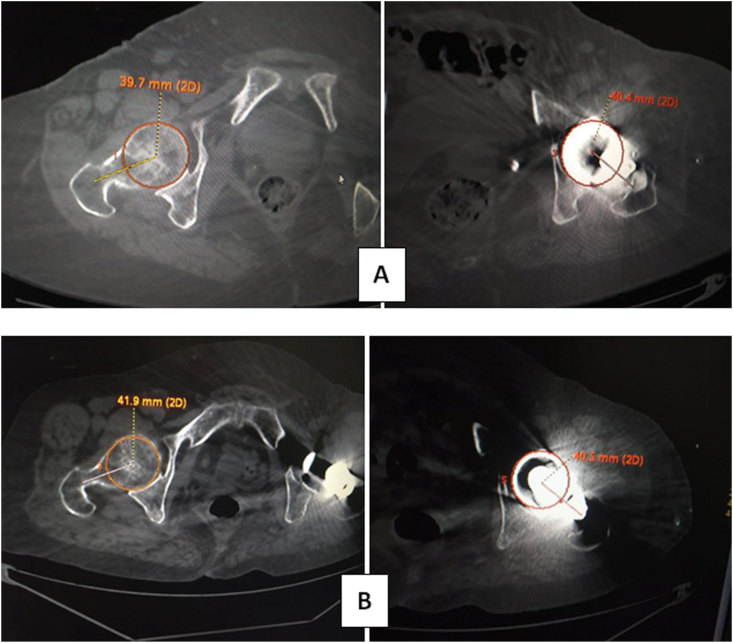
Methods: All active elderly patients with displaced fracture NOF having contralateral normal hip were included. We used an indigenous bicentric bipolar hip-prosthesis, which is a non-modular single-piece device in all cases by lateral Hardinge approach. Postoperative radiograph AP view was taken in 15° internal rotation to decrease the effect of limb rotation on offset. CT scan was also used to evaluate offsets using ADW4.6 ADVANCED GE optima 128 slice software system. Subjects were followed for a minimum of 12 months postoperatively and functional outcome of effect of offsets change were evaluated by modified Harris Hip Score.
Results: There is minimal difference in horizontal and vertical offset after bicentric bipolar hemi-replacement which is statistically insignificant supporting our hypothesis. The clinical outcomes were good to fair according to modified Harris Hip Score. The mean value of horizontal offset after our bipolar hemireplacement was 42.4 ± 2.04 mm and of normal hip was 41.8 ± 1.81 mm and P-value=0.08 in plain radiographs and value of horizontal offset in CT scan was 40.73 ± 0.27on bipolar side and 41.19 ± 0.77 on normal side. Vertical offset after bicentric bipolar was 32.67 ± 2.85 mm and vertical offset of normal hip was 32.53 ± 2.73 mm. Mean 9.77 ± 1.09 mm of calcar was preserved. Modified Harris Hip Score at 6 and 12 months postoperatively was 75.78 ± 4.16 and 79.53 ± 3.95 respectively. There was no incidence of hip dislocation.
Conclusion: Our study data clearly demonstrates that vertical and horizontal offsets are effectively maintained by the indigenous bicentric hip device. There was insignificant change in offsets as compared to contralateral normal side due to its design modifications. Indigenous bicentric non-modular bipolar device offers an excellent option for femur neck fractures in elderly patients in resource constrained situations. It allows rapid rehabilitation due to reduced surgical time, minimal blood loss and early return to function and activities of daily living.
Keywords: Bicentric; Bipolar; Femur; Fracture; Hemiarthroplasty; Neck; Offset.
© 2020 Delhi Orthopedic Association. All rights reserved.
Conflict of interest statement
There are no conflicts of interest associated with this work.
Figures
Similar articles
-
Does femoral offset recover and affect the functional outcome of patients with displaced femoral neck fracture following hemiarthroplasty?Injury. 2017 Jun;48(6):1170-1174. doi: 10.1016/j.injury.2017.03.022. Epub 2017 Mar 21. Injury. 2017. PMID: 28365072
-
Bicentric bipolar hip prosthesis: A radiological study of movement at the interprosthetic joint.Indian J Orthop. 2011 Nov;45(6):508-13. doi: 10.4103/0019-5413.87120. Indian J Orthop. 2011. PMID: 22144743 Free PMC article.
-
The BHU bicentric bipolar prosthesis in fracture neck femur in active elderly.J Trauma Manag Outcomes. 2008 Sep 25;2(1):7. doi: 10.1186/1752-2897-2-7. J Trauma Manag Outcomes. 2008. PMID: 18817566 Free PMC article.
-
Fractures of the femoral neck: a review and personal statement.Acta Chir Orthop Traumatol Cech. 2006;73(1):45-59. Acta Chir Orthop Traumatol Cech. 2006. PMID: 16613748 Review.
-
Femoral offset: anatomical concept, definition, assessment, implications for preoperative templating and hip arthroplasty.Orthop Traumatol Surg Res. 2009 May;95(3):210-9. doi: 10.1016/j.otsr.2009.03.010. Epub 2009 May 6. Orthop Traumatol Surg Res. 2009. PMID: 19423418 Review.
References
-
- Sassoon A., D’Apuzzo M., Sems S., Cass J., Mabry T. Total hip arthroplasty for femoral neck fracture: comparing in-hospital mortality, complications, and disposition to an elective patient population. J Arthroplasty. 2013;28(9):1659–1662. - PubMed
-
- Cho M.R. Lee HS Early results after the treatment with total hip arthroplasty with larger diameter femoral head versus bipolar arthroplasty in patients with femoral neck fractures. J Korean Hip Soc. 2007;19(4):463–467.
-
- Lecerf G., Fessy M.H., Philippot R. Femoral offset: anatomical concept, definition, assessment, implications for preoperative templating and hip arthroplasty. Orthop Traumatol Surg Res. 2009;95(3):210–219. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources