

Obesity does not influence acetabular component accuracy when using a 3D optical computer navigation system
- PMID: 33717895
- PMCID: PMC7919980
- DOI: 10.1016/j.jcot.2020.09.028
Obesity does not influence acetabular component accuracy when using a 3D optical computer navigation system
Erratum in
-
Erratum regarding previously published articles.J Clin Orthop Trauma. 2021 Aug 5;21:101558. doi: 10.1016/j.jcot.2021.101558. eCollection 2021 Oct. J Clin Orthop Trauma. 2021. PMID: 34414072 Free PMC article.
Abstract
Introduction: Improper cup positioning and leg length discrepancy (LLD) are two of the most common errors following total hip arthroplasty (THA) and are associated with potentially significant consequences. Obesity is associated with increased risk of mechanical complications, including dislocations, which may be secondary to cup malposition and failure to restore leg length and offset. 3D Optical Camera computerassisted navigation (CAN) system may reduce the risk of component malposition and LLD with real time intraoperative feedback. The aim of this study was to investigate whether the use of CAN influences acetabular component placement (CP) accuracy and leg length restoration in obese (body mass index(BMI)≥35kg/m 2 ) patients undergoing primary THA.
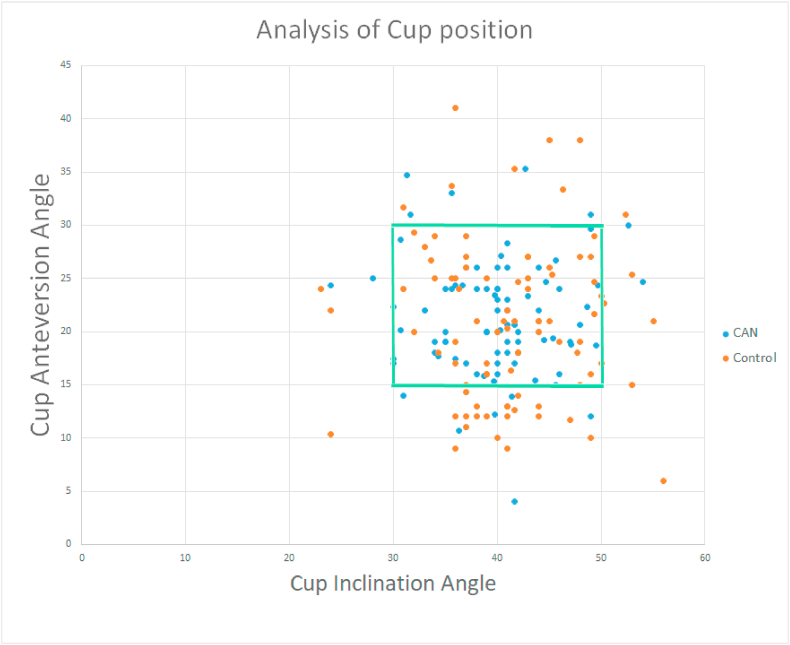
Methods: A multi-center retrospective review was conducted identifying consecutive THA cases with BMI > 35kg/m 2 using CAN (Intellijoint Hip, Waterloo, CA) from 2015-2019. These patients were then matched with patients undergoing conventional THA (control) at a 1:1 ratio according to BMI, American Society of Anesthesiologists score, and gender. TraumaCad™ software (Brainlab, Chicago, IL) was used to measure cup anteversion, inclination, and change (Δ) in LLD between pre- and postoperative radiographic images. The safety target zones used as reference for precision analysis of CP were 15°-30° for anteversion and 30°-50° for inclination.
Results: 176 patients were included: 88 CAN and 88 control cases. CAN cases were found to have a lower ΔLLD than controls (3.53±2.12mm vs. 5.00±4.05mm; p=0.003). Additionally, more CAN cases fell within the target safe zone than controls (83% vs.60%, p=0.00083).
Conclusion: Our findings suggest that the use of a CAN system may be more precise in component placement, and useful in facilitating the successful restoration of preoperative leg length following THA than conventional methodology.
© 2020 Delhi Orthopedic Association. All rights reserved.
Figures
References
-
- Lewinnek G.E., Lewis J.L., Tarr R., Compere C.L., Zimmerman J.R. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978;60(2):217–220. - PubMed
-
- Nishii T., Sugano N., Miki H., Koyama T., Takao M., Yoshikawa H. Influence of component positions on dislocation: computed tomographic evaluations in a consecutive series of total hip arthroplasty. J Arthroplasty. 2004;19(2):162–166. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous