

Active vs passive haptic feedback technology in virtual reality arthroscopy simulation: Which is most realistic?
- PMID: 33717962
- PMCID: PMC7920125
- DOI: 10.1016/j.jcot.2021.02.014
Active vs passive haptic feedback technology in virtual reality arthroscopy simulation: Which is most realistic?
Erratum in
-
Erratum regarding previously published articles.J Clin Orthop Trauma. 2021 Jul 30;20:101539. doi: 10.1016/j.jcot.2021.101539. eCollection 2021 Sep. J Clin Orthop Trauma. 2021. PMID: 34405084 Free PMC article.
Abstract
Background: Virtual Reality (VR) simulators are playing an increasingly prominent role in orthopaedic training and education. Face-validity - the degree to which reality is accurately represented - underpins the value of a VR simulator as a learning tool for trainees. Despite the importance of tactile feedback in arthroscopy, there is a paucity for evidence regarding the role of haptics in VR arthroscopy simulator realism.
Purpose: To assess the difference in face validity between two high fidelity VR simulators employing passive and active haptic feedback technology respectively.
Method: 38 participants were recruited and divided into intermediate and expert groups based on orthopaedic training grade. Each participant completed a 12-point diagnostic knee arthroscopy VR module using the active haptic Simbionix ARTHRO Mentor and passive haptic VirtaMed ArthroS simulators. Subsequently, each participant completed a validated simulator face validity questionnaire.
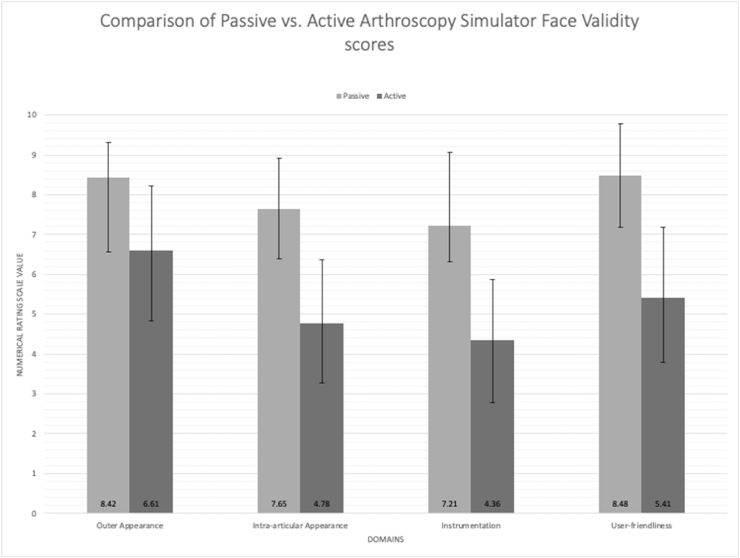
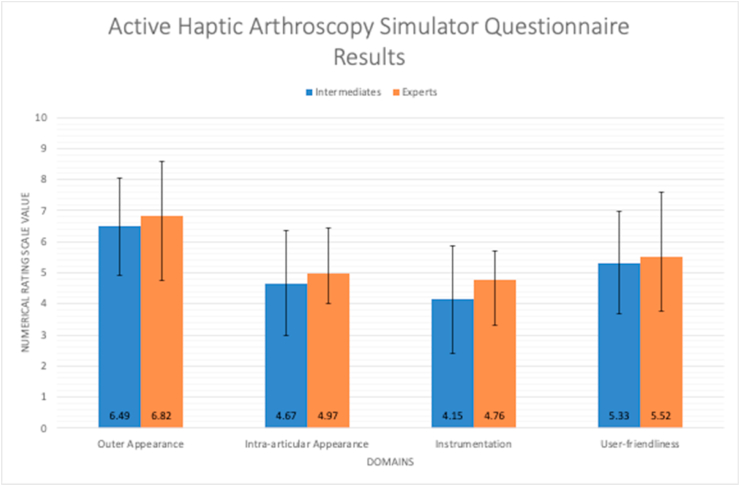
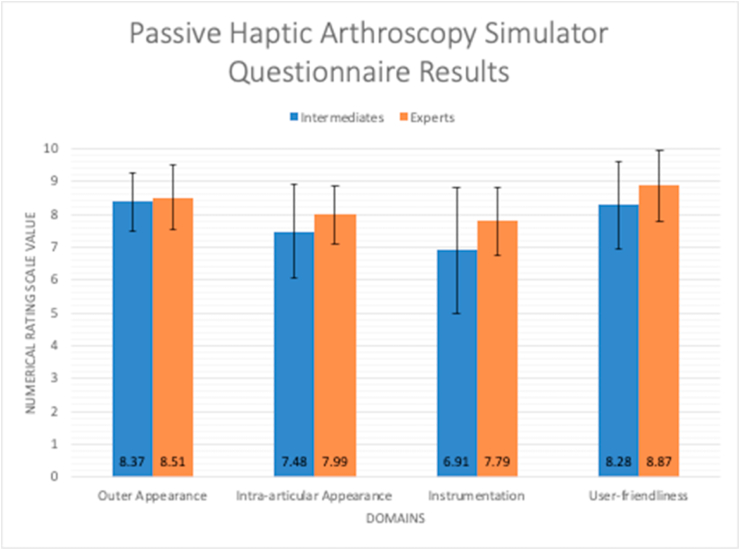
Results: The ARTHRO Mentor active haptic system failed to achieve face validity with mean scores for external appearance (6.61), intra-articular appearance (4.78) and instrumentation (4.36) falling below the acceptable threshold (≥7.0). The ArthroS passive haptic simulator demonstrated satisfactory scores in all domains: external appearance (8.42), intra-articular appearance (7.65), instrumentation (7.21) and was significantly (p < 0.001) more realistic than ARTHRO Mentor for all metrics. 61% of participants gave scores ≥7.0 for questions pertaining to haptic feedback realism from intra-articular structures such as menisci and ACL/PCL for the ArthroS vs. 12% for ARTHRO Mentor. There was no difference in face-validity perception between intermediate and expert groups for either simulator (p > 0.05).
Conclusion: Current active haptic technology which employs motors to simulate tactile feedback fails to demonstrate sufficient face-validity or match the sophistication of passive haptic systems in high fidelity arthroscopy simulators. Textured rubber phantoms that mirror the anatomy and haptic properties of the knee joint provide a significantly more realistic training experience for both intermediate and expert arthroscopists.
Keywords: Arthroscopy; Simulation; Training; Virtual reality.
© 2021 Delhi Orthopedic Association. All rights reserved.
Figures


References
-
- Gmc . 2019. The State of Medical Education and Practice in the UK.
-
- Wilson T., Sahu A., Johnson D.S., Turner P.G. The effect of trainee involvement on procedure and list times: a statistical analysis with discussion of current issues affecting orthopaedic training in UK. Surgeon. 2010;8:15–19. - PubMed
-
- Kim S., Bosque J., Meehan J.P., Jamali A., Marder R. Increase in outpatient knee arthroscopy in the United States: a comparison of national surveys of ambulatory surgery, 1996 and 2006. J Bone Joint Surg Am. 2011;93:994–1000. - PubMed
-
- Irani J.L., Mello M.M., Ashley S.W., Whang E.E., Zinner M.J., Breen E. Surgical residents’ perceptions of the effects of the ACGME duty hour requirements 1 year after implementation. Surgery. 2005;138:246–253. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources