

Wearable robotic exoskeleton for gait reconstruction in patients with spinal cord injury: A literature review
- PMID: 33717982
- PMCID: PMC7930505
- DOI: 10.1016/j.jot.2021.01.001
Wearable robotic exoskeleton for gait reconstruction in patients with spinal cord injury: A literature review
Abstract
Objectives: Wearable robotic exoskeletons (WREs) have been globally developed to achieve gait reconstruction in patients with spinal cord injury (SCI). The present study aimed to enable evidence-based decision-making in selecting the optimal WRE according to residual motor function and to provide a new perspective on further development of appropriate WREs.
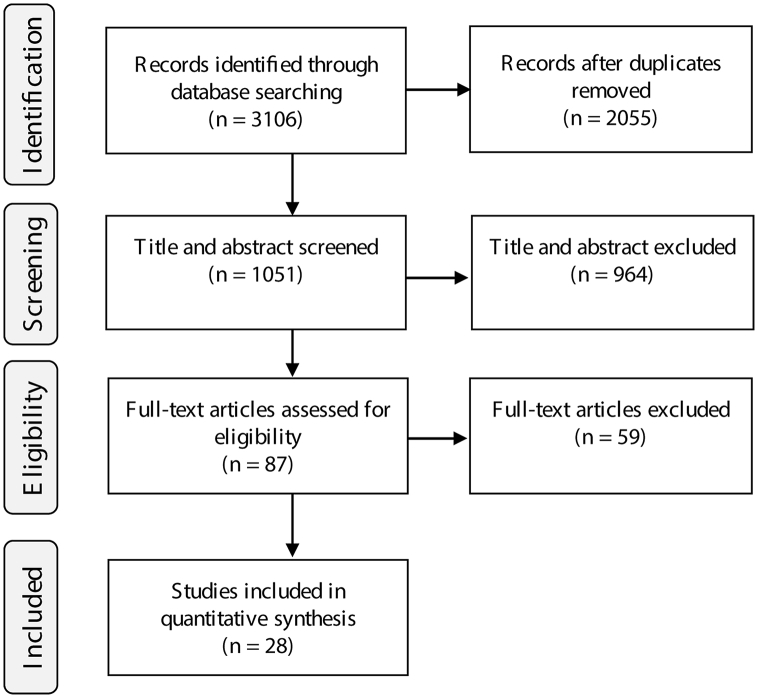
Methods: The current review was conducted by searching PubMed, Web of Science, and Google Scholar for relevant studies published from April 2015 to February 2020. Selected studies were analysed with a focus on the participants' neurological level of SCI, amount of training (number of training sessions and duration of the total training period), gait speed and endurance achieved, and subgroup exploration of the number of persons for assistance and the walking aid used among patients with cervical level injury.
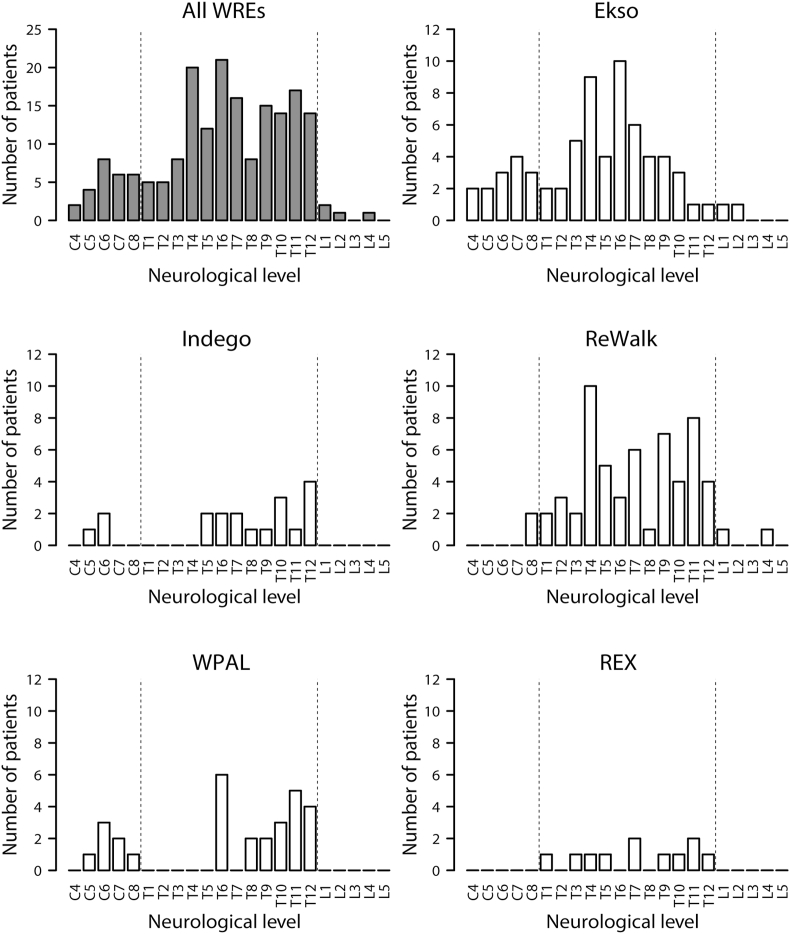
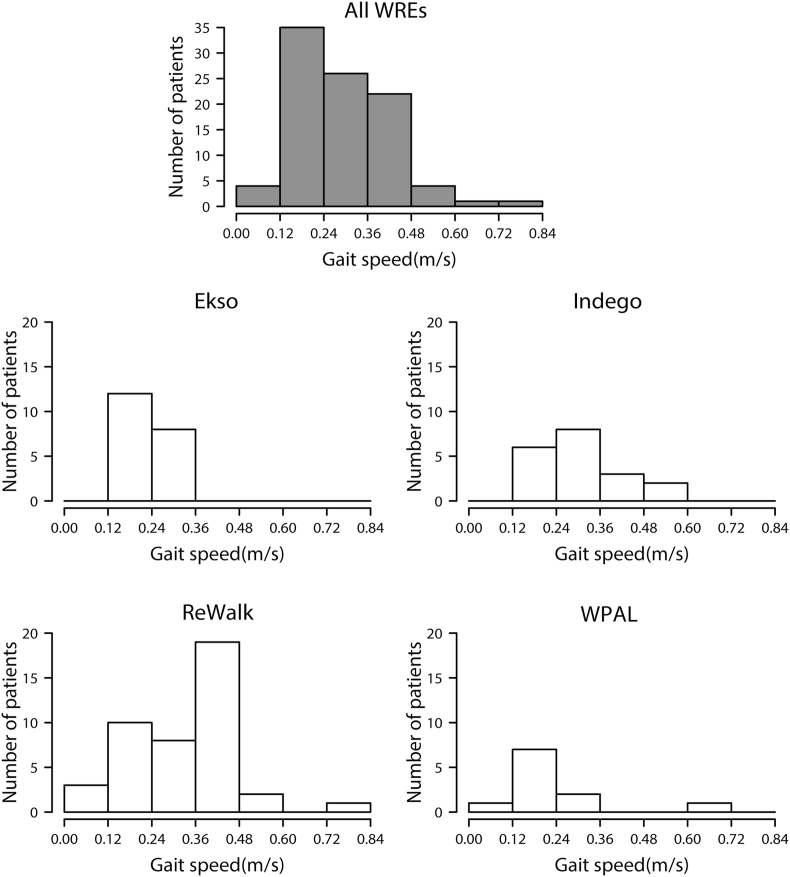
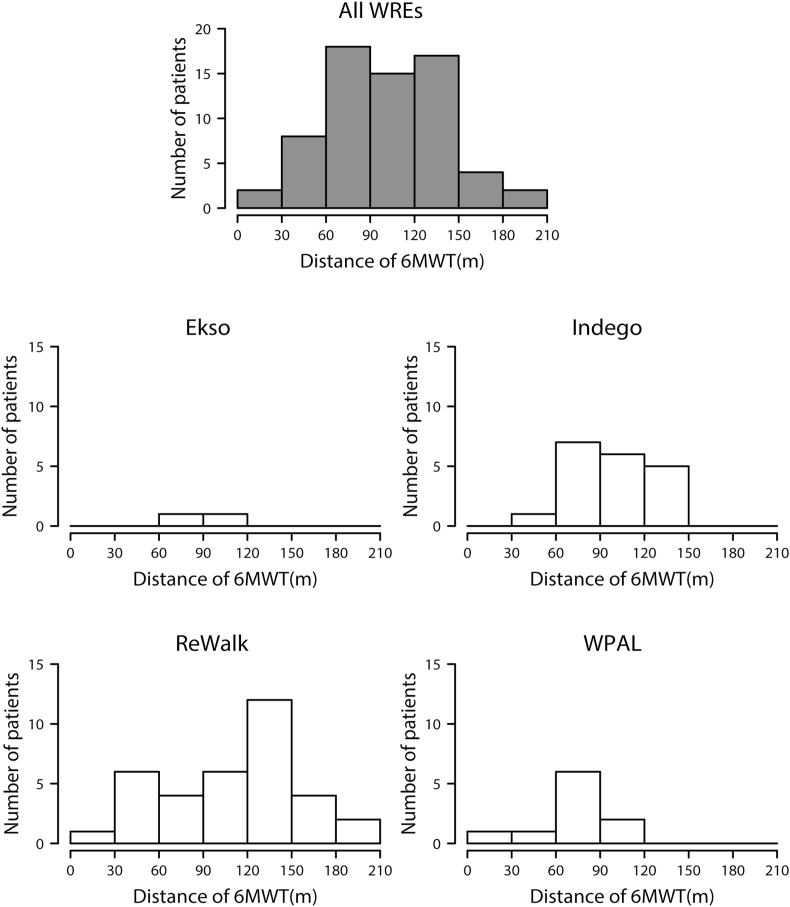
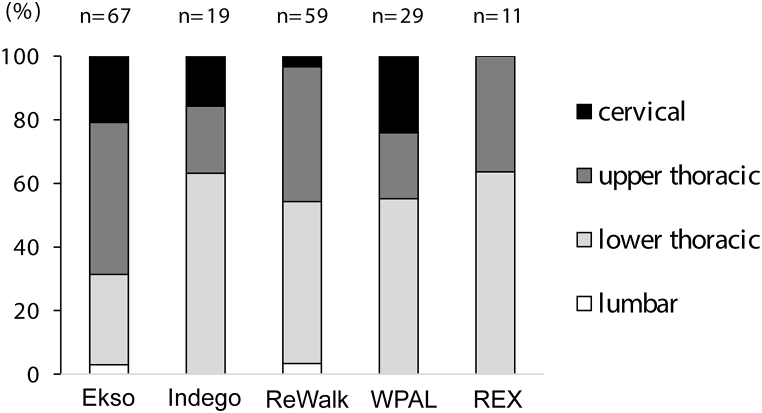
Results: A total of 28 articles (nine using Ekso, three using Indego, ten using ReWalk, one using REX, five using Wearable Power-Assist Locomotor) involving 228 patients were included in the analysis. Across all WREs, T6 was the most frequently reported level of SCI. The amount of training showed a wide distribution (number of training sessions: 2-230 sessions [30-120 min per session]; duration of the total training period: 1-24 weeks [1-5 times per week]). The mean gait speed was 0.31 m/s (standard deviation [SD] 0.14), and the mean distance on the 6-min walking test as a measure of endurance was 108.9 m (SD 46.7). The subgroup exploration aimed at patients with cervical level injury indicated that 59.2% of patients were able to ambulate with no physical assistance and several patients used a walker as a walking aid.
Conclusion: The number of cervical level injury increased, as compared to the number previously indicated by a prior similar review. Training procedure was largely different among studies. Further improvement based on gait performance is required for use and dissemination in daily life.
The translational potential of this article: The present review reveals the current state of the clinical effectiveness of WREs for gait reconstruction in patients with SCI, contributing to evidence-based device application and further development.
Keywords: Gait reconstruction; Paraplegia; Tetraplegia; Wearable robotic exoskeleton.
© 2021 The Authors.
Conflict of interest statement
The authors have no conflicts of interest relevant to this article.
Figures
References
-
- Jazayeri S.B., Beygi S., Shokraneh F., Hagen E.M., Rahimi-Movaghar V. Incidence of traumatic spinal cord injury worldwide: a systematic review. Eur Spine J. 2015;24:905–918. - PubMed
-
- National Spinal Cord Injury Statistical Center . University of Alabama at Birmingham; Birmingham, AL: 2020. Facts and figures at a glance.https://www.nscisc.uab.edu/Public/Facts and Figures 2020.pdf Available at:
-
- Sakai H., Ueta T., Shiba K. Current situation of medical care for spinal cord injury in Japan. J Spine Res. 2010;1:41–51.
-
- Shingu H., Ohama M., Ikata T., Katoh S., Akatsu T. A nationwide epidemiological survey of spinal cord injuries in Japan from January 1990 to December 1992. Paraplegia. 1995;33:183–188. - PubMed
-
- Kudo D., Miyakoshi N., Hongo M., Kasukawa Y., Ishikawa Y., Ishikawa N. An epidemiological study of traumatic spinal cord injuries in the fastest aging area in Japan. Spinal Cord. 2019;57:509–515. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
