

Evaluating the impact of surgical supply cost variation during partial nephrectomy on patient outcomes
- PMID: 33718078
- PMCID: PMC7947437
- DOI: 10.21037/tau-20-1050
Evaluating the impact of surgical supply cost variation during partial nephrectomy on patient outcomes
Abstract
Background: Reducing surgical supply costs can help to lower hospital expenditures. We aimed to evaluate whether variation in supply costs between urologic surgeons performing both robotic or open partial nephrectomies is associated with differential patient outcomes.
Methods: In this retrospective cohort study, we reviewed 399 consecutive robotic (n=220) and open (n=179) partial nephrectomies performed at an academic center. Surgical supply costs were determined at the institution-negotiated rate. Through retrospective review, we identified factors related to case complexity, patient comorbidity, and perioperative outcomes. Two radiologists assigned nephrometry scores to grade tumor complexity. We created univariate and multivariable models for predictors of supply costs, length of stay, and change in serum creatinine.
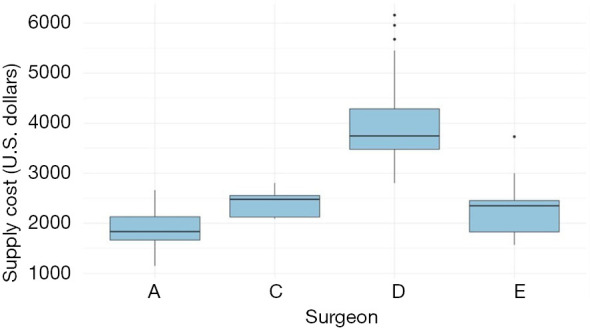
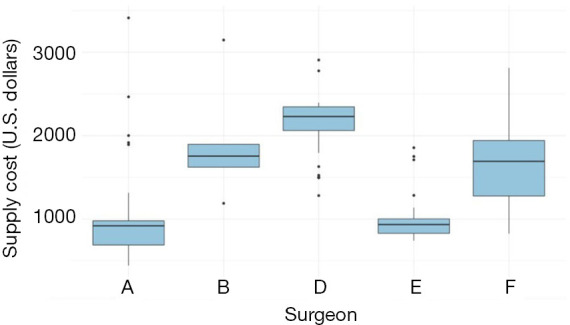
Results: Median supply cost was $3,201 [interquartile range (IQR): $2,201-3,808] for robotic partial nephrectomy and $968 (IQR: $819-1,772) for open partial nephrectomy. Mean nephrometry score was 7.0 (SD =1.7) for robotic procedures and 8.2 (SD =1.6) for open procedures. In multivariable models, the surgeon was the primary significant predictor of variation in surgical supply costs for both procedure types. In multivariable mixed-effects analysis with surgeon as a random effect, supply cost was not a significant predictor of change in serum creatinine for robotic or open procedures. Supply cost was not a statistically significant predictor of length of stay for the open procedure. Supply cost was a significant predictor of longer length of stay for the robotic procedure, however it was not a clinically meaningful change in length of stay (0.02 days per $100 in supply costs).
Conclusions: Higher supply spending did not predict significantly improved patient outcomes. Variability in surgeon supply preference is the likely source of variability in supply cost. These data suggest that efforts to promote cost-effective utilization and standardization of supplies in partial nephrectomy could help reduce costs without harming patients.
Keywords: Cost analysis; partial nephrectomy; quality improvement; surgical supplies; urologic oncology.
2021 Translational Andrology and Urology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tau-20-1050). The authors have no conflicts of interest to declare.
Figures
References
-
- Martin AB, Hartman M, Washington B, et al. National health care spending in 2017: growth slows to post-great recession rates; share of GDP stabilizes. Health Aff (Millwood) 2019;38:101377hlthaff201805085. - PubMed
-
- Wennberg JE. Practice variations and health care reform: connecting the dots. Health Aff (Millwood) 2004;Suppl Variation:VAR140-4. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources