

A Prognostic Model for Glioblastoma Patients Treated With Standard Therapy Based on a Prospective Cohort of Consecutive Non-Selected Patients From a Single Institution
- PMID: 33718145
- PMCID: PMC7946965
- DOI: 10.3389/fonc.2021.597587
A Prognostic Model for Glioblastoma Patients Treated With Standard Therapy Based on a Prospective Cohort of Consecutive Non-Selected Patients From a Single Institution
Abstract
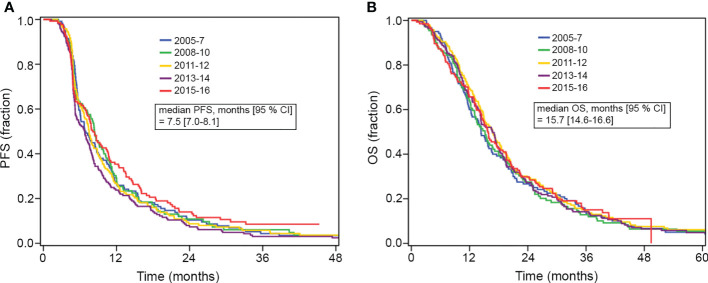
Background: Glioblastoma patients administered standard therapies, comprising maximal surgical resection, radiation therapy with concomitant and adjuvant temozolomide, have a variable prognosis with a median overall survival of 15-16 months and a 2-year overall survival of 30%. The aim of this study was to develop a prognostic nomogram for overall survival for glioblastoma patients treated with standard therapy outside clinical trials.
Methods: The study included 680 consecutive, non-selected glioblastoma patients administered standard therapy as primary treatment between the years 2005 and 2016 at Rigshospitalet, Copenhagen, Denmark. The prognostic model was generated employing multivariate Cox regression analysis modeling overall survival.
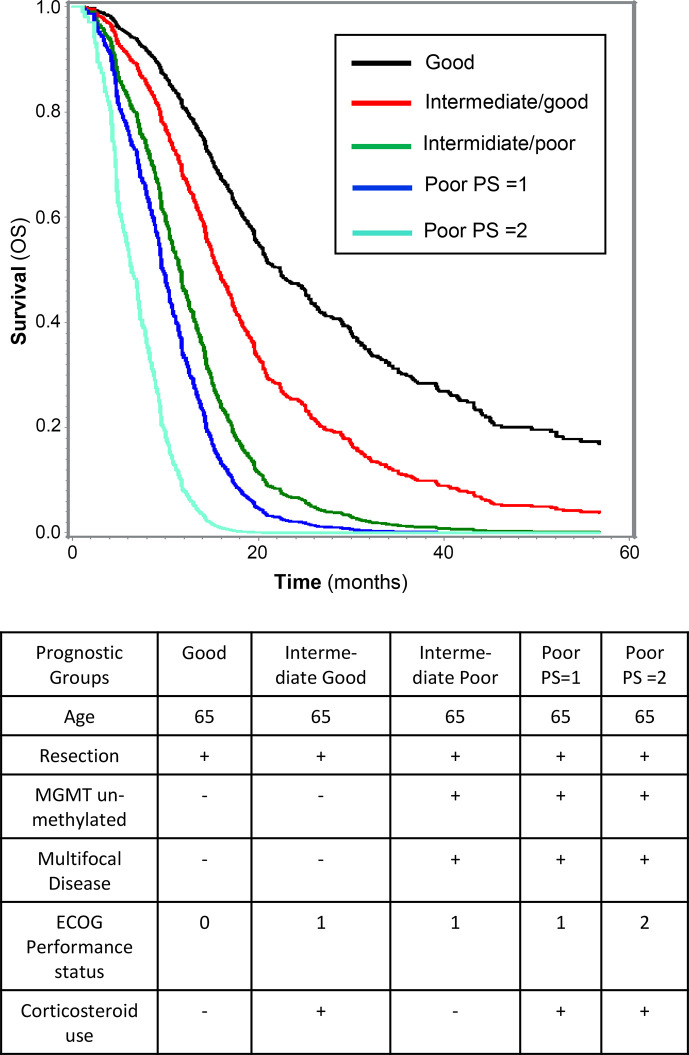
Results: The following poor prognostic factors were included in the final prognostic model for overall survival: Age (10-year increase: HR = 1.18, 95% CI: 1.08-1.28, p < 0.001), ECOG performance status (PS) 1 vs. 0 (HR = 1.30, 95% CI: 1.07-1.57, p = 0.007), PS 2 vs. 0 (HR = 2.99, 95% CI: 1.99-4.50, p < 0.001), corticosteroid use (HR = 1.42, 95% CI: 1.18-1.70, p < 0.001), multifocal disease (HR = 1.63, 95% CI: 1.25-2.13, p < 0.001), biopsy vs. resection (HR = 1.35, 95% CI: 1.04-1.72, p = 0.02), un-methylated promoter of the MGMT (O6-methylguanine-DNA methyltransferase) gene (HR = 1.71, 95% CI: 1.42-2.04, p < 0.001). The model was validated internally and had a concordance index of 0.65.
Conclusion: A nomogram for overall survival was established. This model can be used for risk stratification and treatment planning, as well as improve enrollment criteria for clinical trials.
Keywords: MGMT = O6-DNA-methylguanine methyltransferase; biomarkers; glioblastoma; glioma grade IV; nomogram; overall survival; prognostic factors; progression-free survival.
Copyright © 2021 Abedi, Grunnet, Christensen, Michaelsen, Muhic, Møller, Hasselbalch, Poulsen and Urup.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Gittleman H, Lim D, Kattan MW, Chakravarti A, Gilbert MR, Lassman AB, et al. An independently validated nomogram for individualized estimation of survival among patients with newly diagnosed glioblastoma: NRG Oncology RTOG 0525 and 0825. Neuro Oncol (2017) 19(5):669–77. 10.1093/neuonc/now208 - DOI - PMC - PubMed
-
- Nava F, Tramacere I, Fittipaldo A, Bruzzone MG, Dimeco F, Fariselli L, et al. Survival effect of first- and second-line treatments for patients with primary glioblastoma: a cohort study from a prospective registry, 1997-2010. Neuro Oncol (2014) 16(5):719–27. 10.1093/neuonc/not316 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials