

Is Additional Systematic Biopsy Necessary in All Initial Prostate Biopsy Patients With Abnormal MRI?
- PMID: 33718240
- PMCID: PMC7952882
- DOI: 10.3389/fonc.2021.643051
Is Additional Systematic Biopsy Necessary in All Initial Prostate Biopsy Patients With Abnormal MRI?
Abstract
Purpose: To determine whether additional systematic biopsy is necessary in all biopsy naïve patients with MRI visible lesions by taking PI-RADS score and prostate volume into consideration.
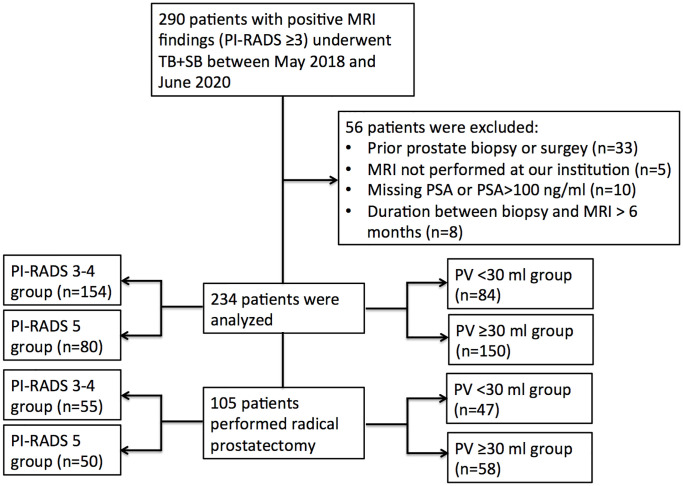
Materials and methods: Patients who underwent combined systematic biopsy (SB) and cognitive MRI-targeted biopsy (TB) in our hospital between May 2018 and June 2020 were retrospectively reviewed. The detection rate of clinical significant prostate cancer (csPCa), biopsy grade group (GG) concordance, and disease upgrading rate on radical prostatectomy were compared between SB and TB and further stratified by PI-RADS v2.0 category and prostate volume.
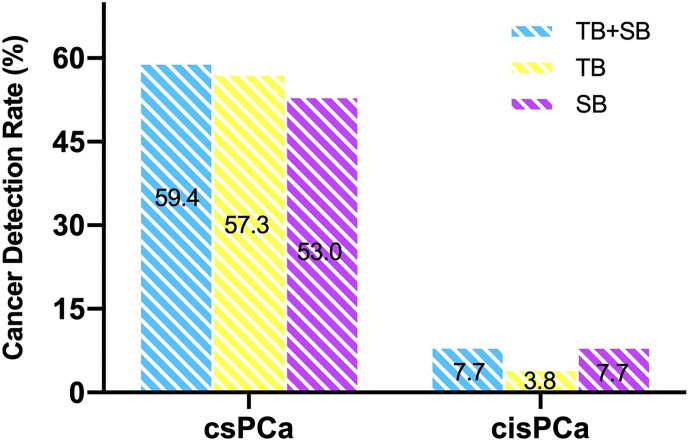
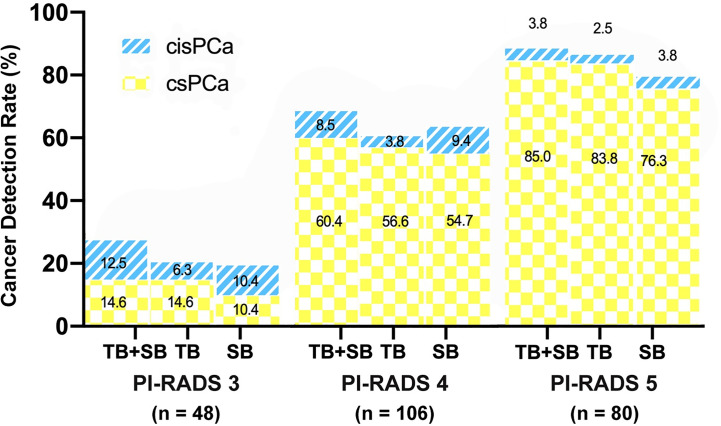
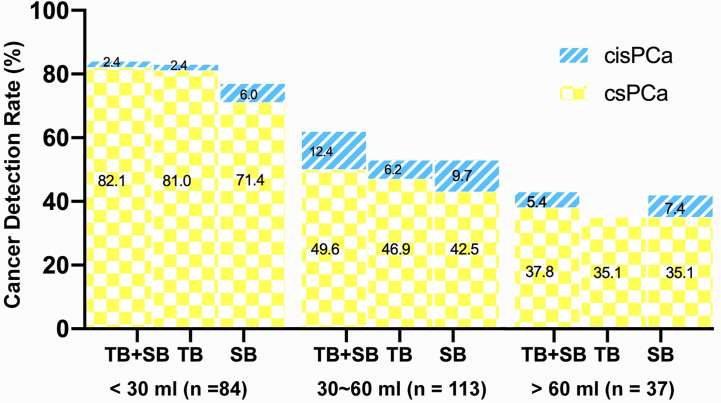
Results: A total of 234 patients were analyzed in this study. TB alone detected more csPCa and less clinically insignificant prostate cancer (cisPCa) than SB alone in the whole cohort (57.3 vs 53%, P = 0.041; 3.8 vs 7.7%, P = 0.049 respectively). The additional SB indicated only a marginal increase of csPCa detection but a remarkable increase of cisPCa detection compared with targeted biopsy (59.4 vs 57.3%, P = 0.064; 3.8 vs 7.7%, P = 0.012). As stratified by PI-RADS category, the difference of csPCa detection rate between TB and SB was not significant either in PI-RADS 5 subgroup (83.8 vs 76.3%, P = 0.07) or in PI-RADS 3-4 subgroup (43.5 vs 40.9%, P = 1.0). Additional SB decreased the rate of disease upgrading on radical prostatectomy (RP) than TB alone in PI-RADS 3-4 subgroup (14.5 vs 25.5%, P = 0.031) other than PI-RADS 5 subgroup (6 vs 6%, P = 1.0). When stratified by prostate volume (PV), TB alone detected more csPCa than SB in small prostate (PV < 30 ml) group (81.0 vs 71.0%, P = 0.021) but not in large prostate (PV ≥ 30 ml) group (44.0 vs 42.7%, P = 0.754). The additional SB did not significantly decrease the rate of disease upgrading on RP than TB alone in either small or large prostate (6.4 vs 8.5%, P = 1.0; 13.8 vs 22.4%, P = 0.063).
Conclusion: The combination biopsy method was no superior than targeted biopsy alone in PI-RADS 5 or in small volume prostate subgroup.
Keywords: MRI; PI-RADS; prostate biopsy; prostate cancer; targeted biopsy.
Copyright © 2021 Cheng, Xu, Chen, Liu, Sun, Yang, Yao, Zeng and Song.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Combining targeted and systematic prostate biopsy improves prostate cancer detection and correlation with the whole mount histopathology in biopsy naïve and previous negative biopsy patients.Front Surg. 2022 Oct 6;9:1013389. doi: 10.3389/fsurg.2022.1013389. eCollection 2022. Front Surg. 2022. PMID: 36277287 Free PMC article.
-
Diagnostic performance of transperineal prostate targeted biopsy alone according to the PI-RADS score based on bi-parametric magnetic resonance imaging.Front Oncol. 2023 Mar 23;13:1142022. doi: 10.3389/fonc.2023.1142022. eCollection 2023. Front Oncol. 2023. PMID: 37035173 Free PMC article.
-
Is There Still a Need for Repeated Systematic Biopsies in Patients with Previous Negative Biopsies in the Era of Magnetic Resonance Imaging-targeted Biopsies of the Prostate?Eur Urol Oncol. 2020 Apr;3(2):216-223. doi: 10.1016/j.euo.2019.06.005. Epub 2019 Jun 22. Eur Urol Oncol. 2020. PMID: 31239236
-
Diagnostic Role of Magnetic Resonance Imaging-Targeted Biopsy for Prostate Cancer in Biopsy-Naïve Men: A Meta-Analysis.Urol Int. 2020;104(3-4):187-198. doi: 10.1159/000504028. Epub 2019 Dec 11. Urol Int. 2020. PMID: 31825927
-
Is ipsilateral systematic biopsy combined with targeted biopsy the optimal substitute for bilateral systematic biopsy combined with targeted biopsy: A systematic review and meta-analysis.Urol Oncol. 2025 May;43(5):307-317. doi: 10.1016/j.urolonc.2024.11.023. Epub 2024 Dec 21. Urol Oncol. 2025. PMID: 39710538
Cited by
-
Sextant Systematic Biopsy Versus Extended 12-Core Systematic Biopsy in Combined Biopsy for Prostate Cancer.J Korean Med Sci. 2024 Feb 26;39(7):e63. doi: 10.3346/jkms.2024.39.e63. J Korean Med Sci. 2024. PMID: 38412610 Free PMC article.
-
Prostate Biopsy in the Case of PIRADS 5-Is Systematic Biopsy Mandatory?J Clin Med. 2023 Aug 28;12(17):5612. doi: 10.3390/jcm12175612. J Clin Med. 2023. PMID: 37685679 Free PMC article.
-
Development and validation of a predictive model based on clinical and MpMRI findings to reduce additional systematic prostate biopsy.Insights Imaging. 2024 Jan 7;15(1):3. doi: 10.1186/s13244-023-01544-0. Insights Imaging. 2024. PMID: 38185753 Free PMC article.
References
-
- Siddiqui MM, Rais-Bahrami S, Truong H, Stamatakis L, Vourganti S, Nix J, et al. . Magnetic Resonance Imaging/Ultrasound–Fusion Biopsy Significantly Upgrades Prostate Cancer Versus Systematic 12-core Transrectal Ultrasound Biopsy. Eur Urol (2013) 64(5):713–9. 10.1016/j.eururo.2013.05.059 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous