

Objective Assessment of Physiologic Alterations Associated With Hemodynamically Significant Patent Ductus Arteriosus in Extremely Premature Neonates
- PMID: 33718311
- PMCID: PMC7946992
- DOI: 10.3389/fped.2021.648584
Objective Assessment of Physiologic Alterations Associated With Hemodynamically Significant Patent Ductus Arteriosus in Extremely Premature Neonates
Abstract
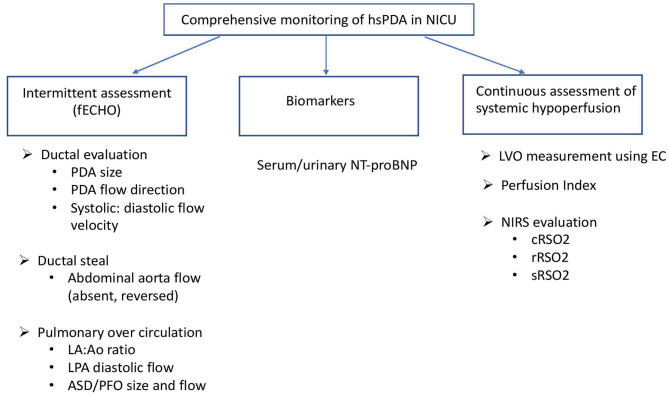
Delay in closure of ductus arteriosus in postnatal life may lead to serious consequences and complications in an extremely premature neonate secondary to hemodynamic alterations in regional blood flow pattern in various organs. Despite the widespread recognition amongst neonatologists to identify a hemodynamically significant patent ductus arteriosus (hsPDA) early in the postnatal course, there is lack of consensus in its definition and thus the threshold to initiate treatment. Echocardiographic assessment of PDA shunt size and volume combined with neonatologists' impression of clinical significance is most frequently used to determine the need for treatment of PDA. Common clinical signs of hsPDA utilized as surrogate for decreased tissue perfusion may lag behind early echocardiographic signs. Although echocardiogram allows direct assessment of PDA shunt and hemodynamic alterations in the heart, it is limited by dependence on pediatric cardiologist availability, interobserver variation and isolated time point assessment. Electrical cardiometry (EC) is a non-invasive continuous real time measurement of cardiac output by applying changes in thoracic electrical impedance. EC has been validated in preterm newborns by concomitant transthoracic echocardiogram assessments and may be beneficial in studying changes in cardiac output in premature newborns with hsPDA. Alterations in perfusion index derived from continuous pulse oximetry monitoring has been used to study changes in cardiac performance and tissue perfusion in infants with PDA. Near infrared spectroscopy (NIRS) has been used to objectively and continuously assess variations in renal, mesenteric, and cerebral oxygen saturation and thus perfusion changes due to diastolic vascular steal from hsPDA in preterm neonates. Doppler ultrasound studies measuring resistive indices in cerebral circulation indicate disturbance in cerebral perfusion secondary to ductal steal. With recent trends of change in practice toward less intervention in care of preterm newborn, treatment strategy needs to be targeted for select preterm population most vulnerable to adverse hemodynamic effects of PDA. Integration of these novel ways of hemodynamic and tissue perfusion assessment in routine clinical care may help mitigate the challenges in defining and targeting treatment of hsPDA thereby improving outcomes in extremely premature neonates.
Keywords: echocardiogram; electrical cardiometry; hsPDA; near-infrared spectroscopy; physiologic; preterm.
Copyright © 2021 Patra, Thakkar, Makhoul and Bada.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources