

Sex-Specific Patterns of Mortality Predictors Among Patients Undergoing Cardiac Resynchronization Therapy: A Machine Learning Approach
- PMID: 33718444
- PMCID: PMC7947699
- DOI: 10.3389/fcvm.2021.611055
Sex-Specific Patterns of Mortality Predictors Among Patients Undergoing Cardiac Resynchronization Therapy: A Machine Learning Approach
Abstract
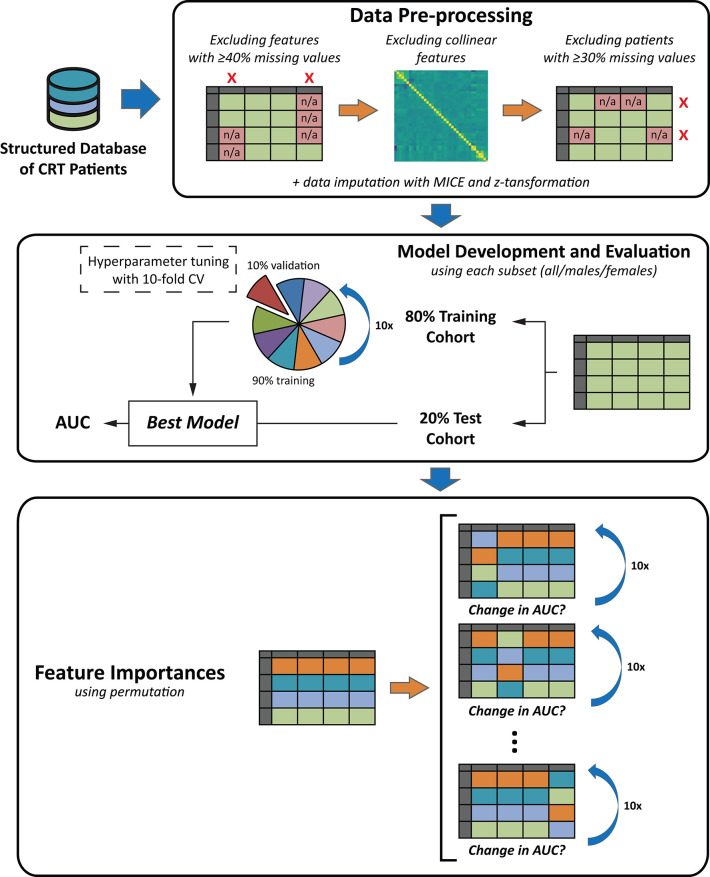
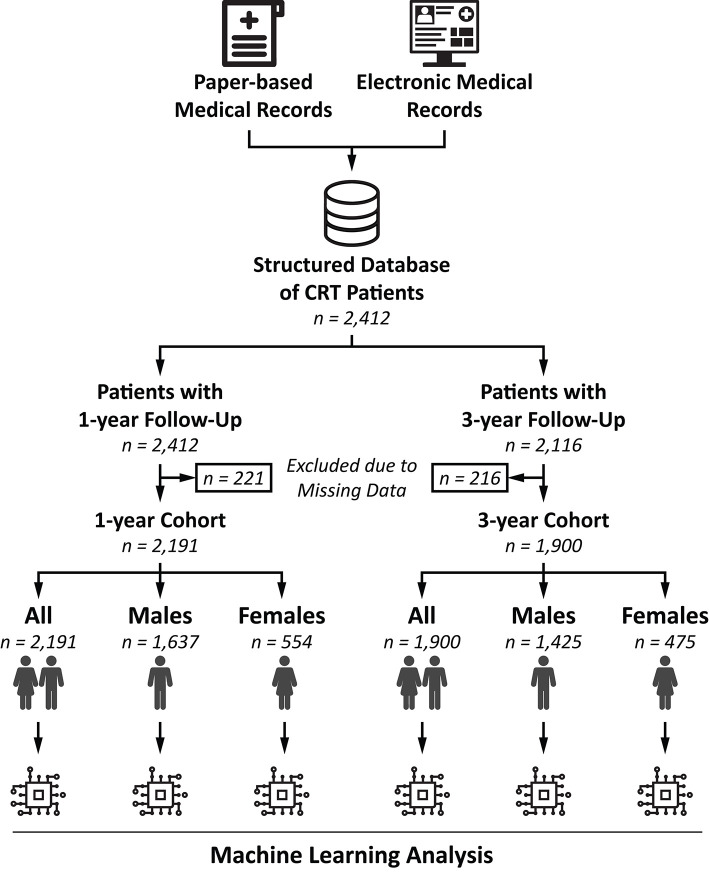
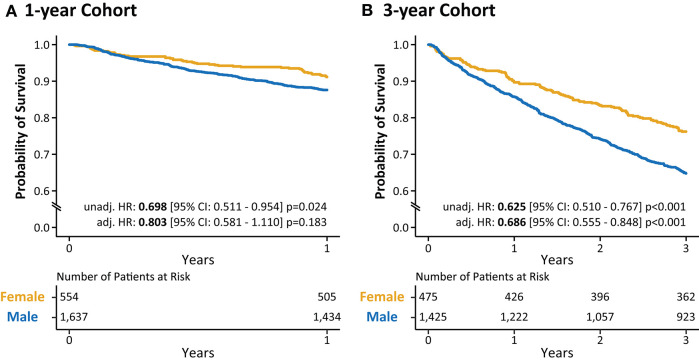
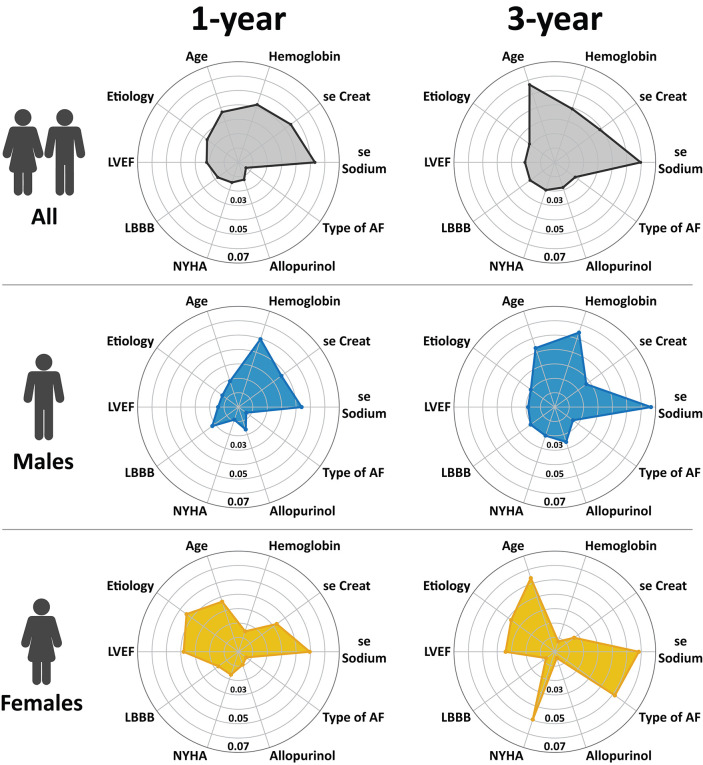
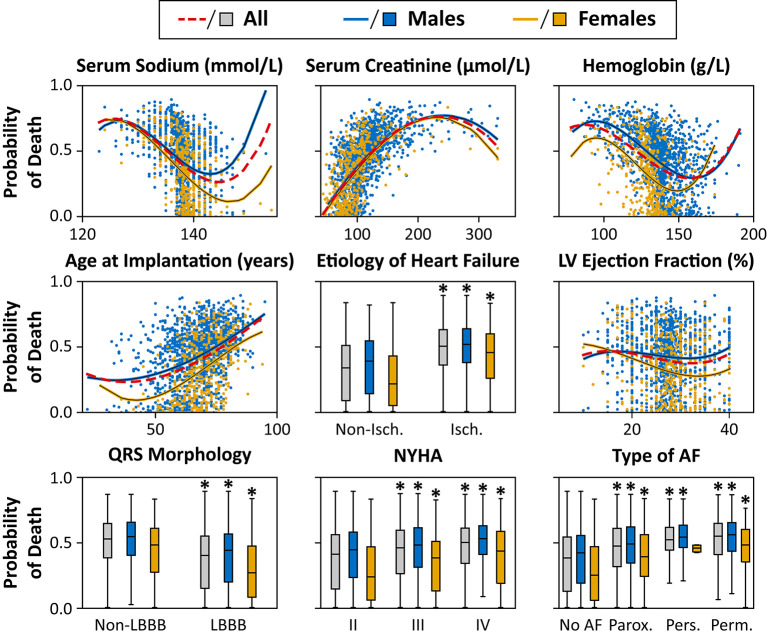
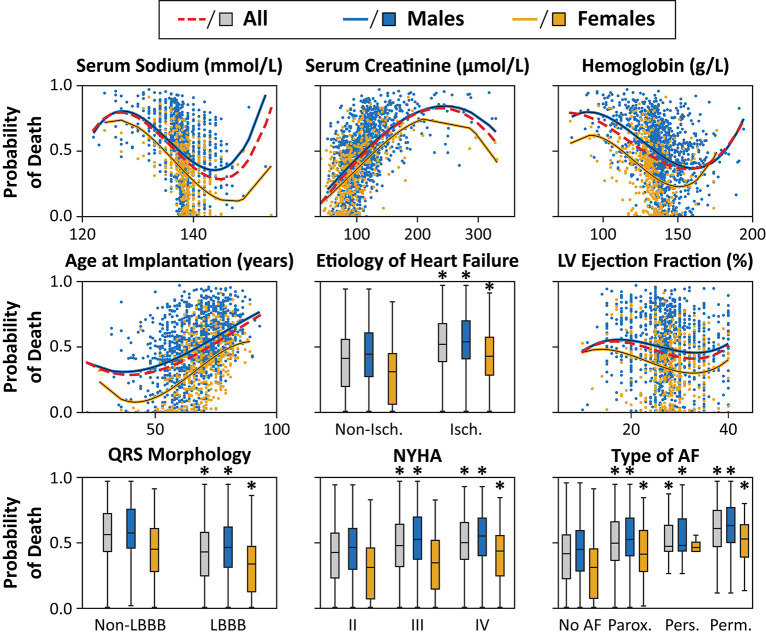
Background: The relative importance of variables explaining sex-related differences in outcomes is scarcely explored in patients undergoing cardiac resynchronization therapy (CRT). We sought to implement and evaluate machine learning (ML) algorithms for the prediction of 1- and 3-year all-cause mortality in CRT patients. We also aimed to assess the sex-specific differences in predictors of mortality utilizing ML. Methods: Using a retrospective registry of 2,191 CRT patients, ML models were implemented in 6 partially overlapping patient subsets (all patients, females, or males with 1- or 3-year follow-up). Each cohort was randomly split into training (80%) and test sets (20%). After hyperparameter tuning in the training sets, the best performing algorithm was evaluated in the test sets. Model discrimination was quantified using the area under the receiver-operating characteristic curves (AUC). The most important predictors were identified using the permutation feature importances method. Results: Conditional inference random forest exhibited the best performance with AUCs of 0.728 (0.645-0.802) and 0.732 (0.681-0.784) for the prediction of 1- and 3-year mortality, respectively. Etiology of heart failure, NYHA class, left ventricular ejection fraction, and QRS morphology had higher predictive power, whereas hemoglobin was less important in females compared to males. The importance of atrial fibrillation and age increased, while the importance of serum creatinine decreased from 1- to 3-year follow-up in both sexes. Conclusions: Using ML techniques in combination with easily obtainable clinical features, our models effectively predicted 1- and 3-year all-cause mortality in CRT patients. Sex-specific patterns of predictors were identified, showing a dynamic variation over time.
Keywords: cardiac resynchronization therapy; heart failure; machine learning; mortality prediction; sex differences.
Copyright © 2021 Tokodi, Behon, Merkel, Kovács, Tősér, Sárkány, Csákvári, Lakatos, Schwertner, Kosztin and Merkely.
Conflict of interest statement
BM receives lecture fees from Biotronik, Medtronic, and Abbott. ZT is a co-founder and CEO of Argus Cognitive, Inc., holds equity in the company, and receives financial compensation for his work. AS and MC are employees of Argus Cognitive, Inc., and receive compensation for their work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Machine Learning Prediction of Response to Cardiac Resynchronization Therapy: Improvement Versus Current Guidelines.Circ Arrhythm Electrophysiol. 2019 Jul;12(7):e007316. doi: 10.1161/CIRCEP.119.007316. Epub 2019 Jun 20. Circ Arrhythm Electrophysiol. 2019. PMID: 31216884 Free PMC article.
-
Machine learning-based mortality prediction of patients undergoing cardiac resynchronization therapy: the SEMMELWEIS-CRT score.Eur Heart J. 2020 May 7;41(18):1747-1756. doi: 10.1093/eurheartj/ehz902. Eur Heart J. 2020. PMID: 31923316 Free PMC article.
-
Determinants of mortality in patients undergoing cardiac resynchronization therapy: baseline clinical, echocardiographic, and angioscintigraphic evaluation prior to resynchronization.Pacing Clin Electrophysiol. 2005 Dec;28(12):1260-70. doi: 10.1111/j.1540-8159.2005.00266.x. Pacing Clin Electrophysiol. 2005. PMID: 16403157
-
Assessment of mechanical dyssynchrony in cardiac resynchronization therapy.Dan Med J. 2014 Dec;61(12):B4981. Dan Med J. 2014. PMID: 25441737 Review.
-
The interaction of sex, height, and QRS duration on the effects of cardiac resynchronization therapy on morbidity and mortality: an individual-patient data meta-analysis.Eur J Heart Fail. 2018 Apr;20(4):780-791. doi: 10.1002/ejhf.1133. Epub 2018 Jan 4. Eur J Heart Fail. 2018. PMID: 29314424 Review.
Cited by
-
Interpretable machine learning predicts cardiac resynchronization therapy responses from personalized biochemical and biomechanical features.BMC Med Inform Decis Mak. 2022 Oct 31;22(1):282. doi: 10.1186/s12911-022-02015-0. BMC Med Inform Decis Mak. 2022. PMID: 36316772 Free PMC article.
-
Combination of personalized computational modeling and machine learning for optimization of left ventricular pacing site in cardiac resynchronization therapy.Front Physiol. 2023 Jul 11;14:1162520. doi: 10.3389/fphys.2023.1162520. eCollection 2023. Front Physiol. 2023. PMID: 37497440 Free PMC article.
-
Machine learning-based prediction of 1-year all-cause mortality in patients undergoing CRT implantation: validation of the SEMMELWEIS-CRT score in the European CRT Survey I dataset.Eur Heart J Digit Health. 2024 Jul 12;5(5):563-571. doi: 10.1093/ehjdh/ztae051. eCollection 2024 Sep. Eur Heart J Digit Health. 2024. PMID: 39318695 Free PMC article.
-
Artificial Intelligence in Heart Failure: Friend or Foe?Life (Basel). 2024 Jan 19;14(1):145. doi: 10.3390/life14010145. Life (Basel). 2024. PMID: 38276274 Free PMC article. Review.
-
Evaluation of machine learning methods for prediction of heart failure mortality and readmission: meta-analysis.BMC Cardiovasc Disord. 2025 Apr 7;25(1):264. doi: 10.1186/s12872-025-04700-0. BMC Cardiovasc Disord. 2025. PMID: 40189534 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials