

Review
doi: 10.3389/fcvm.2021.638399.
eCollection 2021.
Multimodality Imaging in Transcatheter Mitral Interventions
Affiliations
- PMID: 33718458
- PMCID: PMC7950542
- DOI: 10.3389/fcvm.2021.638399
Item in Clipboard
Review
Multimodality Imaging in Transcatheter Mitral Interventions
Front Cardiovasc Med.
.
Abstract
Multimodality imaging is of imperative value for the planning and guidance of transcatheter mitral valve interventions. This review employs the value of different imaging modalities and future implications for clinical practice.
Keywords: echocardigraphy; mitral valve; multimodality imaging; transcatheter repair; transcatheter replacement.
Copyright © 2021 Nikolou, Bilkhu, Kafil, Demetrescu, Kotta, Lucchese, Tzemos and Grapsa.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Transcatheter mitral valve interventions: available devices to date.

Pre-procedural assessment. LV, left ventricular; LVEF, left ventricular ejection fraction; GLS, global longitudinal strain; LA, left atrial; RVEF, right ventricular ejection fraction; LAA, left atrial appendage.
Pre-procedural evaluation for MitraClip: clockwise imaging: (a) mid-esophageal view 0 degrees demonstrating severe mitral regurgitation (b) 3D-TEE surgical view with a posterior cleft like indentation (c) mid-esophageal view 90 degrees—commissural view: severe mitral regurgitation (d) 3D-TEE with color demonstrating the regurgitation through the coaptation gap (e) continuous wave Doppler across mitral valve (f) pulmonary vein signal—pulsed wave Doppler.

(Left) Tranesophageal echocardiography at 140 degrees for the evaluation of severe mitral regurgitation—(right) MitraClip positioning and 3D- transesophageal surgical view.

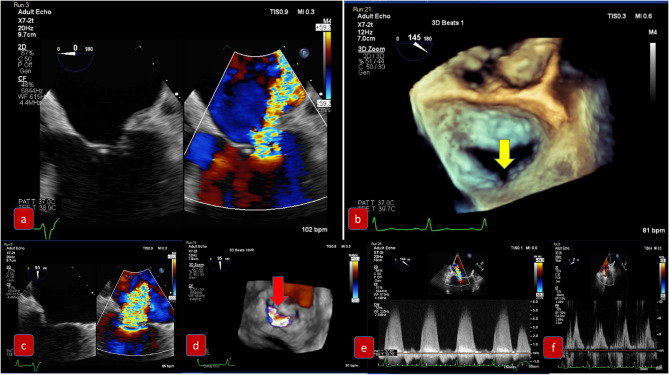
Pre-procedural evaluation for paravalvular leak due to degenerative rocking of a mitral prosthesis: (a) mid-esophageal view 90 degrees demonstrating severe paravalvular mitral regurgitation (b) 3D-TEE surgical view with slight detachment of the prosthetic valve from the suture line and posterolateral gap (c) Continuous wave Doppler of severe mitral regurgitation (d) 3D-TEE with color demonstrating the regurgitation (e) pulmonary vein signal—pulsed wave Doppler.

Post-procedural assessment. MVR, mitral valve replacement; PFO, patent foramen ovale; 3D, 3-dimensional; EROA, effective orifice area; CW, continuous wave; MV, mitral valve.

Algorithm to guide implementation of integration of multiple parameters of MR severity after mitral valve percutaneous interventions (with permission from JASE).

Cardiac MRI. Functional mitral regurgitation planning for mitral valve clip. (a) SSFP Cine 4-chamber showing severely dilated left ventricular cavity with “tented” mitral valve leaflets and evidence of significant mitral regurgitation (arrow) into a dilated left atrium. (b) SSFP Cine short axis of the mitral valve closure showing the jet of mitral regurgitation mostly confined toward the posterior annulus (arrow).

Cardiac MRI. Planning of alcohol septal ablation in patient with hypertrophic cardiomyopathy and severe mitral regurgitation due to systolic movement of the anterior mitral valve leaflet (SAM). (a) SSFP-cine Three chamber: Systolic motion of the anterior MV with intracavitary flow acceleration (diphasic) and consequent significant mitral regurgitation. Asymmetrical septal hypertrophy. (b) T1-weighted late gadolinium enhancement (LGE-MRI) Short axis mid ventricular showing late gadolinium hyperenhancement of the papillary muscle-chordal apparatus (arrow) due to fibrosis secondary to traumatic contact with the septum.
References
-
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, III, Gentile F, et al. . (2020). ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. J Am Coll Cardiol. (2020) 143:e35–71. 10.1161/CIR.0000000000000932 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources