

Pulmonary hypertension in eosinophilic versus noneosinophilic COPD
- PMID: 33718496
- PMCID: PMC7938054
- DOI: 10.1183/23120541.00772-2020
Pulmonary hypertension in eosinophilic versus noneosinophilic COPD
Abstract
Background: The eosinophilic COPD phenotype is associated with greater airway remodelling, exacerbation risk and steroid responsiveness. However, little is known about the prevalence and characteristics of pulmonary hypertension (PH) in this patient population.
Methods: We retrospectively evaluated a cohort of COPD patients with right heart catheterisation (RHC) data at a university hospital between January 2011 and May 2019 and compared the pulmonary vascular profile and prevalence of PH between eosinophilic and noneosinophilic patients using a definition of eosinophilic COPD as at least three blood eosinophil values ≥300 cells·µL-1. We used multivariable logistic regression analyses to examine the association between eosinophilic COPD and various PH categories adjusting for age, sex, body mass index, forced expiratory volume in 1 s (%), smoking status and use of supplemental oxygen.
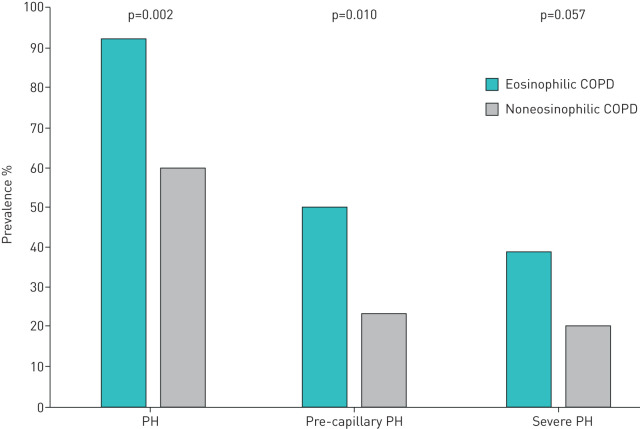
Results: Among 106 COPD patients with RHC data and at least three blood eosinophil values, 25% met the definition of eosinophilic COPD. Fewer patients among the eosinophilic group required long-term oxygen therapy (69% versus 93%, p=0.001) and total lung capacity was significantly lower in the eosinophilic group (p=0.006). This group had higher mean pulmonary arterial pressure (mPAP) (median (interquartile range) 30 (27-41) mmHg versus 25 (22-30) mmHg, p=0.001) and pulmonary vascular resistance (PVR) (4 (2.8-5.1) Wood units versus 2.9 (2.1-4.1) Wood units, p=0.018). On multivariable logistic regression analyses, eosinophilic phenotype was associated with PH (adjusted (a)OR 6.5, 95% CI 1.4-30.7; p=0.018) and pre-capillary PH (aOR 3.2, 95% CI 1.1-9; p=0.027), but not severe PH (aOR 2.1, 95% CI 0.6-7.2; p=0.219).
Conclusion: Eosinophilic COPD was associated with higher mPAP and PVR and increased likelihood of PH. More studies are needed to further explore this finding.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: B.N. Alzghoul has nothing to disclose. Conflict of interest: M. As Sayaideh has nothing to disclose. Conflict of interest: B.F. Moreno has nothing to disclose. Conflict of interest: S.K. Singh has nothing to disclose. Conflict of interest: A. Innabi has nothing to disclose. Conflict of interest: R. Reddy has nothing to disclose. Conflict of interest: E.S. Papierniak has nothing to disclose. Conflict of interest: H.M. Alnuaimat has nothing to disclose.
Figures
References
-
- World Health Organization (WHO). Global Health Estimates. www.who.int/healthinfo/global_burden_disease/en/ Date last accessed: 31 August 2020.
-
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management and Prevention of COPD. 2020. Available from: www.goldcopd.org/ - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous