

Progressive Monoarticular Inflammatory Arthritis Following Influenza Vaccination
- PMID: 33718794
- PMCID: PMC7930781
- DOI: 10.1016/j.mayocpiqo.2020.08.004
Progressive Monoarticular Inflammatory Arthritis Following Influenza Vaccination
Abstract
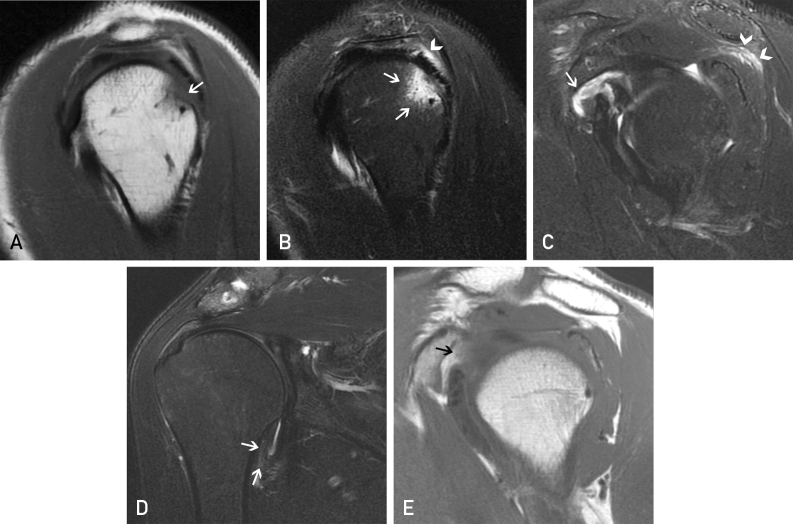
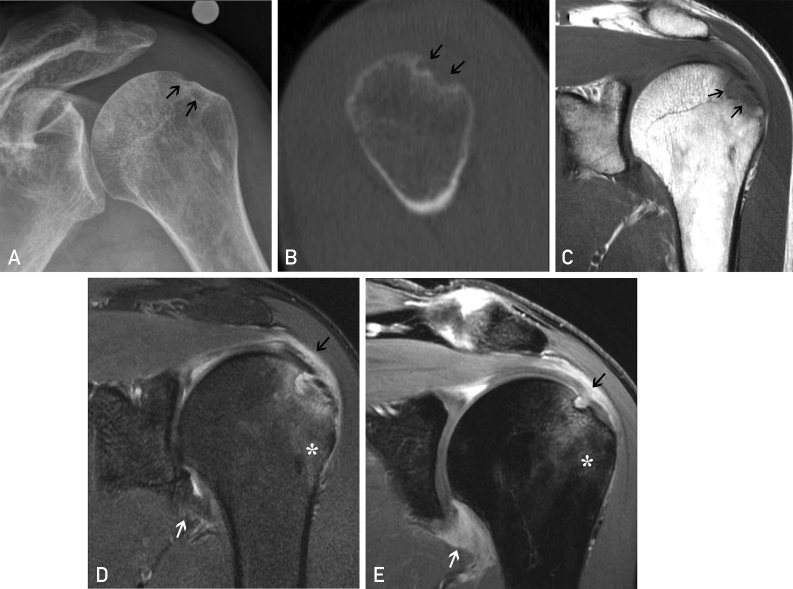
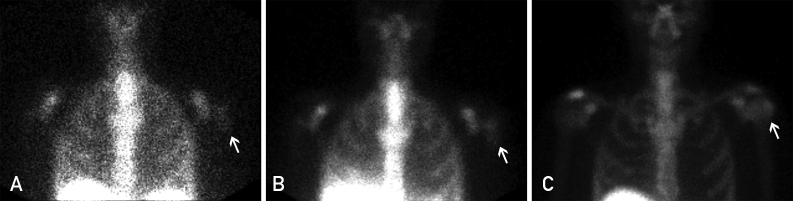
Musculoskeletal injury is an uncommon but usually self-limited complication of vaccine administration. We present a case of progressive inflammatory monoarthritis of the shoulder characterized by bone erosion, bursitis, and severe synovitis caused by an influenza vaccine administered to the ipsilateral deltoid region. Clinical symptoms began within 2 hours of vaccination, with progressive decline in function over 6 weeks. Magnetic resonance imaging examinations performed 5 months apart demonstrated progressive erosive changes of the greater tuberosity, rotator cuff injury, and extensive enhancing synovitis of the glenohumeral joint and subacromial/subdeltoid bursa. After the exclusion of septic arthritis and osteomyelitis, the patient underwent nonoperative treatment and experienced near-complete recovery at 32 months. Although inflammatory arthritis of the shoulder following vaccination is rare, there have been previous reports of it. Clinicians and radiologists need to be aware of this potential complication to ensure an accurate diagnosis.
Keywords: CT, computed tomography; MRI, magnetic resonance imaging.
© 2020 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc.
Figures
References
-
- Historical Reference of Seasonal Influenza Vaccine Doses Distributed. https://www.cdc.gov/flu/prevent/vaccinesupply.htm Available at:
-
- 2017-2018 Estimated Influenza Illnesses, Medical visits, and Hospitalizations Averted by Vaccination in the United States. https://www.cdc.gov/flu/vaccines-work/averted-estimates.htm Available at:
-
- The Vaccine Adverse Event Reporting System (VAERS) https://wonder.cdc.gov/vaers.html Available at: - PubMed
-
- Bodor M., Montalvo E. Vaccination-related shoulder dysfunction. Vaccine. 2007;25(4):585–587. - PubMed
-
- Atanasoff S., Ryan T., Lightfoot R., Johann-Liang R. Shoulder injury related to vaccine administration (SIRVA) Vaccine. 2010;28(51):8049–8052. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
