

Prospective Study on Plasma MicroRNA-4286 and Incident Acute Coronary Syndrome
- PMID: 33719498
- PMCID: PMC8174203
- DOI: 10.1161/JAHA.120.018999
Prospective Study on Plasma MicroRNA-4286 and Incident Acute Coronary Syndrome
Abstract
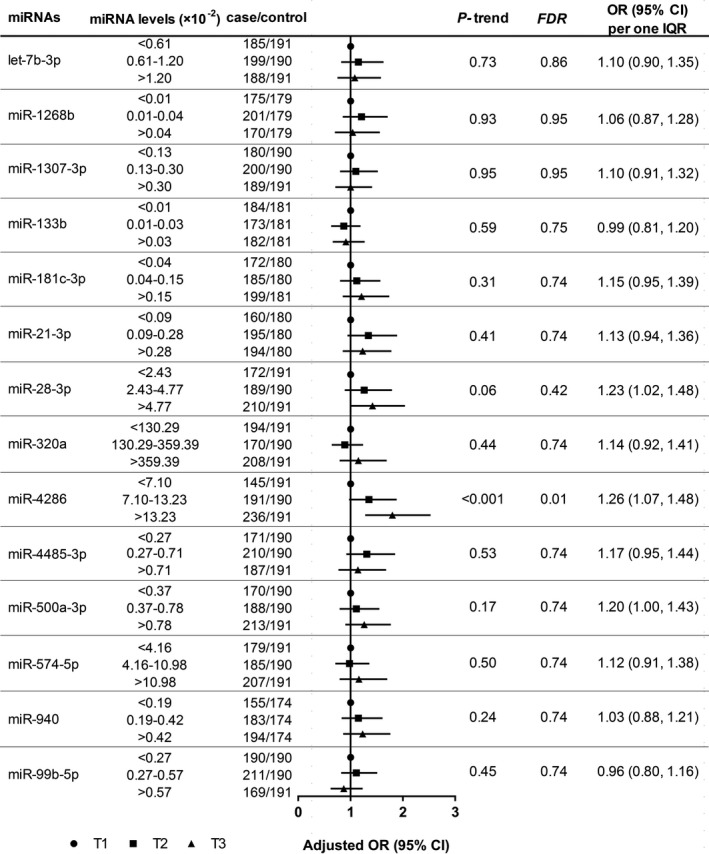
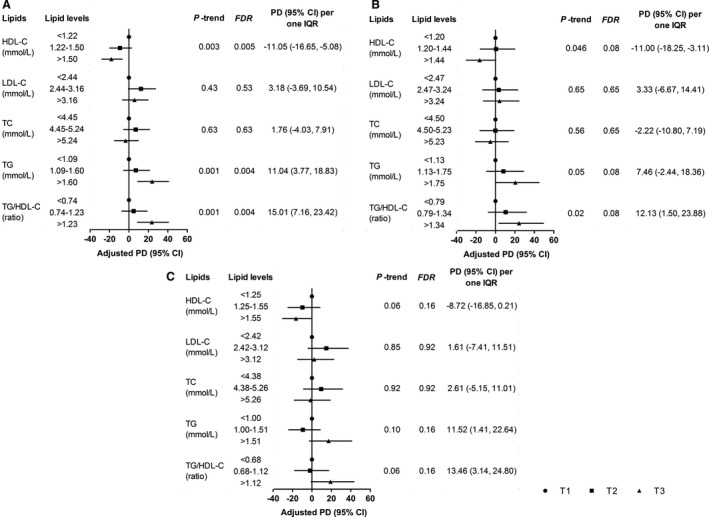
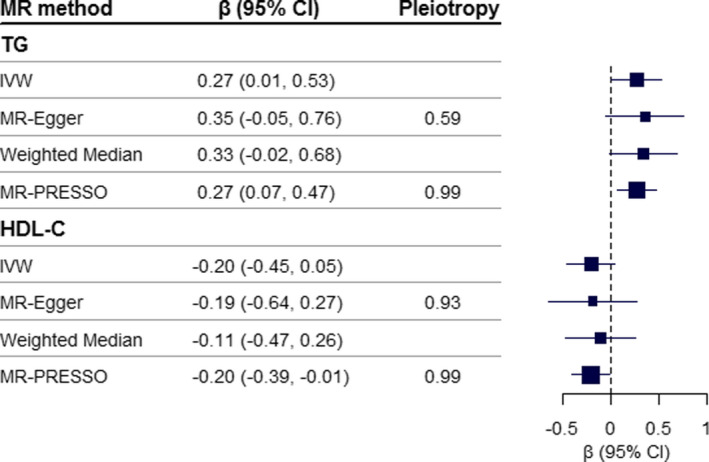
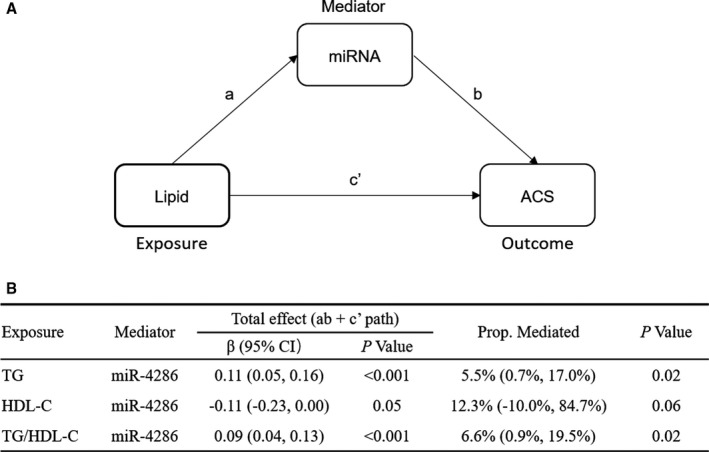
Background Mounting evidence suggests that circulating microRNAs (miRNAs) are critical indicators of cardiovascular disease. However, prospective studies linking circulating miRNAs to incident acute coronary syndrome (ACS) are limited, and the underlying effect of associated miRNA on incident ACS remains unknown. Methods and Results Based on a 2-stage prospective nested case-control design within the Dongfeng-Tongji cohort, we profiled plasma miRNAs from 23 pairs of incident ACS cases and controls by microarray and validated the candidate miRNAs in 572 incident ACS case-control pairs using quantitative real-time polymerase chain reaction. We observed that plasma miR-4286 was associated with higher risk of ACS (adjusted odds ratio according to an interquartile range increase, 1.26 [95% CI, 1.07-1.48]). Further association analysis revealed that triglyceride was positively associated with plasma miR-4286, and an interquartile range increase in triglyceride was associated with an 11.04% (95% CI, 3.77%-18.83%) increase in plasma miR-4286. In addition, the Mendelian randomization analysis suggested a potential causal effect of triglyceride on plasma miR-4286 (β coefficients: 0.27 [95% CI, 0.01-0.53] and 0.27 [95% CI, 0.07-0.47] separately by inverse variance-weighted and Mendelian randomization-pleiotropy residual sum and outlier tests). Moreover, the causal mediation analysis indicated that plasma miR-4286 explained 5.5% (95% CI, 0.7%-17.0%) of the association of triglyceride with incident ACS. Conclusions Higher level of plasma miR-4286 was associated with an increased risk of ACS. The upregulated miR-4286 in plasma can be attributed to higher triglyceride level and may mediate the effect of triglyceride on incident ACS.
Keywords: acute coronary syndrome; miR‐4286; microRNA; prospective study; triglyceride.
Conflict of interest statement
None.
Figures
References
-
- GBD . 2017 Causes of Death Collaborators. Global, regional, and national age‐sex‐specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1736–1788. DOI: 10.1016/S0140-6736(18)32203-7. - DOI - PMC - PubMed
-
- O'Connor RE, Bossaert L, Arntz HR, Brooks SC, Diercks D, Feitosa‐Filho G, Nolan JP, Vanden Hoek TL, Walters DL, Wong A, et al. Part 9: acute coronary syndromes: 2010 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2010;122:S422–S465. DOI: 10.1161/CIRCULATIONAHA.110.985549. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
