

Predictors of Poststroke Aphasia Recovery: A Systematic Review-Informed Individual Participant Data Meta-Analysis
- PMID: 33719515
- PMCID: PMC8078126
- DOI: 10.1161/STROKEAHA.120.031162
Predictors of Poststroke Aphasia Recovery: A Systematic Review-Informed Individual Participant Data Meta-Analysis
Abstract
Background and purpose: The factors associated with recovery of language domains after stroke remain uncertain. We described recovery of overall-language-ability, auditory comprehension, naming, and functional-communication across participants' age, sex, and aphasia chronicity in a large, multilingual, international aphasia dataset.
Methods: Individual participant data meta-analysis of systematically sourced aphasia datasets described overall-language ability using the Western Aphasia Battery Aphasia-Quotient; auditory comprehension by Aachen Aphasia Test (AAT) Token Test; naming by Boston Naming Test and functional-communication by AAT Spontaneous-Speech Communication subscale. Multivariable analyses regressed absolute score-changes from baseline across language domains onto covariates identified a priori in randomized controlled trials and all study types. Change-from-baseline scores were presented as estimates of means and 95% CIs. Heterogeneity was described using relative variance. Risk of bias was considered at dataset and meta-analysis level.
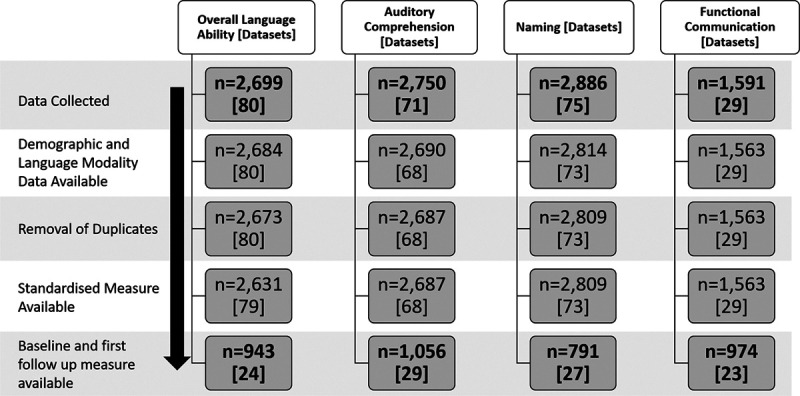
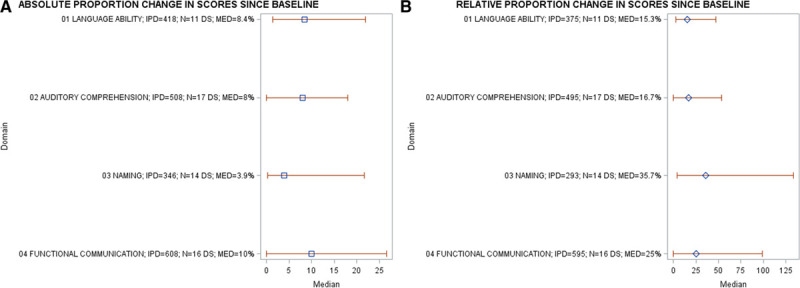
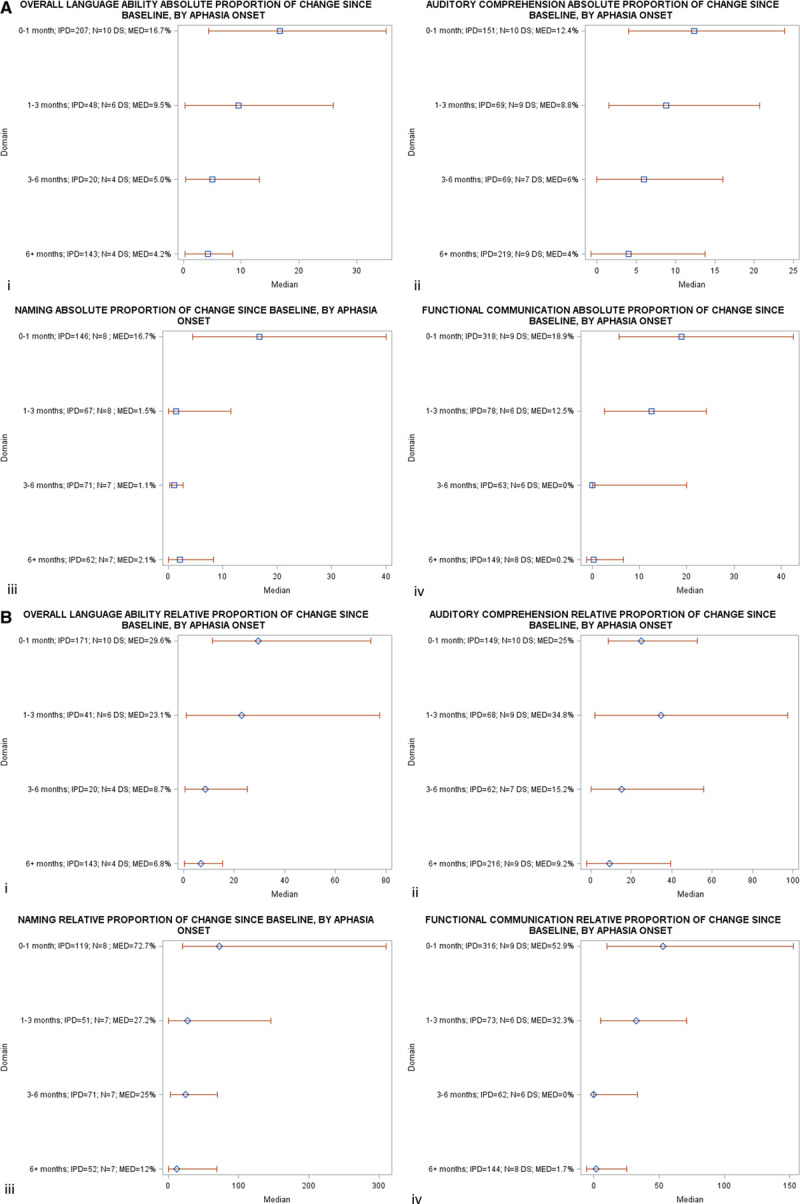
Results: Assessments at baseline (median=43.6 weeks poststroke; interquartile range [4-165.1]) and first-follow-up (median=10 weeks from baseline; interquartile range [3-26]) were available for n=943 on overall-language ability, n=1056 on auditory comprehension, n=791 on naming and n=974 on functional-communication. Younger age (<55 years, +15.4 Western Aphasia Battery Aphasia-Quotient points [CI, 10.0-20.9], +6.1 correct on AAT Token Test [CI, 3.2-8.9]; +9.3 Boston Naming Test points [CI, 4.7-13.9]; +0.8 AAT Spontaneous-Speech Communication subscale points [CI, 0.5-1.0]) and enrollment <1 month post-onset (+19.1 Western Aphasia Battery Aphasia-Quotient points [CI, 13.9-24.4]; +5.3 correct on AAT Token Test [CI, 1.7-8.8]; +11.1 Boston Naming Test points [CI, 5.7-16.5]; and +1.1 AAT Spontaneous-Speech Communication subscale point [CI, 0.7-1.4]) conferred the greatest absolute change-from-baseline across each language domain. Improvements in language scores from baseline diminished with increasing age and aphasia chronicity. Data exhibited no significant statistical heterogeneity. Risk-of-bias was low to moderate-low.
Conclusions: Earlier intervention for poststroke aphasia was crucial to maximize language recovery across a range of language domains, although recovery continued to be observed to a lesser extent beyond 6 months poststroke.
Keywords: aphasia; comprehension; demography; language; survivor.
Figures
Comment in
-
Meta-analysis exploring poststroke aphasia profiles and language recovery.Evid Based Nurs. 2022 Apr;25(2):54. doi: 10.1136/ebnurs-2021-103442. Epub 2021 Aug 20. Evid Based Nurs. 2022. PMID: 34417222 No abstract available.
References
-
- Feigin VL, Norrving B, Mensah GA. Global burden of stroke. Circ Res. 2017;120:439–448. doi: 10.1161/CIRCRESAHA.116.308413 - PubMed
-
- Gialanella B, Bertolinelli M, Lissi M, Prometti P. Predicting outcome after stroke: the role of aphasia. Disabil Rehabil. 2011;33:122–129. doi: 10.3109/09638288.2010.488712 - PubMed
-
- Paolucci S, Antonucci G, Grasso MG, Morelli D, Troisi E, Coiro P, Bragoni M. Early versus delayed inpatient stroke rehabilitation: a matched comparison conducted in Italy. Arch Phys Med Rehabil. 2000;81:695–700. doi: 10.1016/s0003-9993(00)90095-9 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
