

Hybrid Approach to Estimation of Underreporting of Tuberculosis Case Notification in High-Burden Settings With Weak Surveillance Infrastructure: Design and Implementation of an Inventory Study
- PMID: 33720030
- PMCID: PMC8088841
- DOI: 10.2196/22352
Hybrid Approach to Estimation of Underreporting of Tuberculosis Case Notification in High-Burden Settings With Weak Surveillance Infrastructure: Design and Implementation of an Inventory Study
Abstract
Background: The greatest risk of infectious disease undernotification occurs in settings with limited capacity to detect it reliably. World Health Organization guidance on the measurement of misreporting is paradoxical, requiring robust, independent systems to assess surveillance rigor. Methods are needed to estimate undernotification in settings with incomplete, flawed, or weak surveillance systems. This study attempted to design a tuberculosis (TB) inventory study that balanced rigor with feasibility for high-need settings.
Objective: This study aims to design a hybrid TB inventory study for contexts without World Health Organization preconditions. We estimated the proportion of TB cases that were not reported to the Ministry of Health in 2015. The study sought to describe TB surveillance coverage and quality at different levels of TB care provision. Finally, we aimed to identify structural-, facility-, and provider-level barriers to notification and reasons for underreporting, nonreporting, and overreporting.
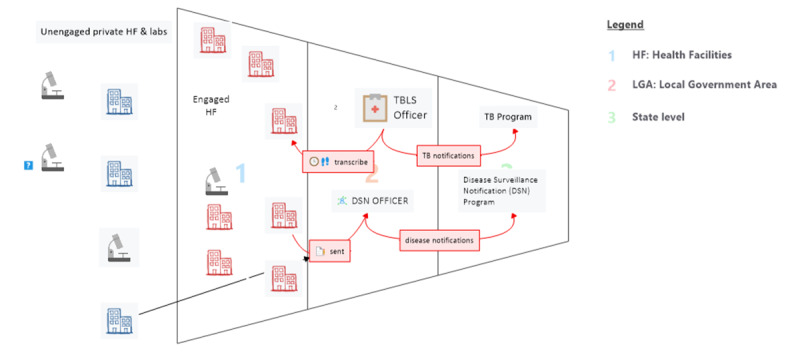
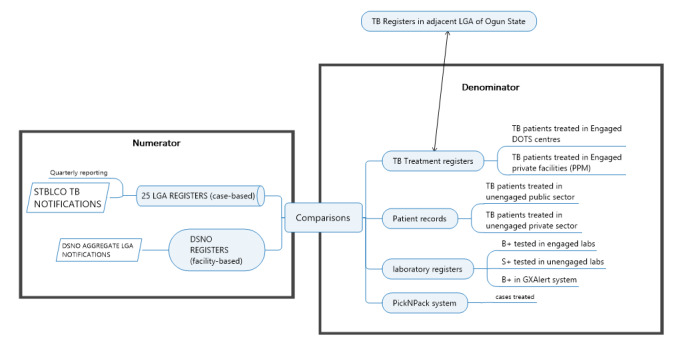
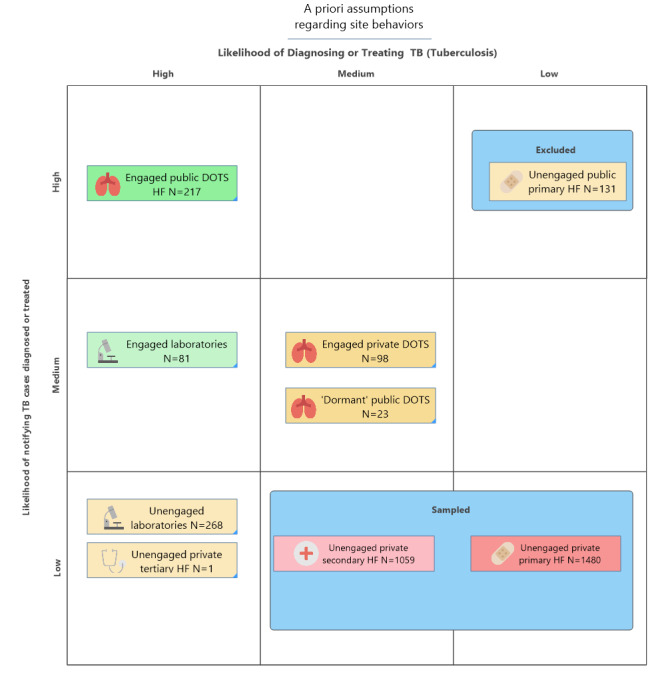
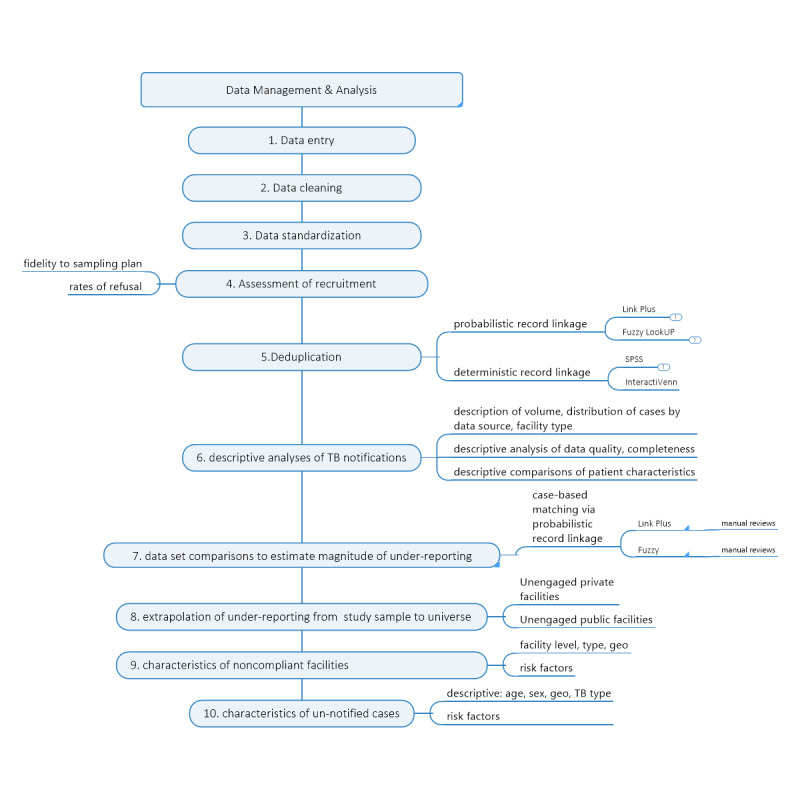
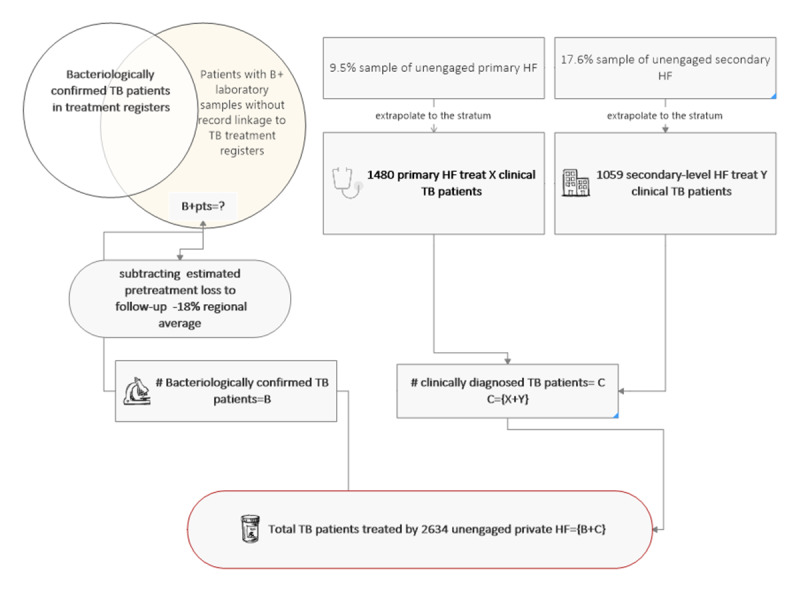
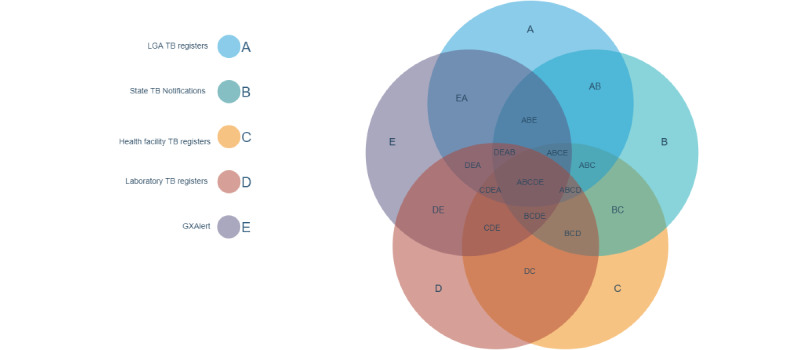
Methods: Retrospective partial digitalization of paper-based surveillance and facility records preceded deterministic and probabilistic record linkage; a hybrid of health facilities and laboratory census with a stratified sampling of HFs with no capacity to notify leveraged a priori knowledge. Distinct extrapolation methods were applied to the sampled health facilities to estimate bacteriologically confirmed versus clinical TB. In-depth interviews and focus groups were used to identify causal factors responsible for undernotification and test the acceptability of remedies.
Results: The hybrid approach proved viable and instructive. High-specificity verification of paper-based records in the field was efficient and had minimal errors. Limiting extrapolation to clinical cases improved precision. Probabilistic record linkage is computationally intensive, and the choice of software influences estimates. Record absence, decay, and overestimation of the private sector TB treatment behavior threaten validity, meriting mitigation. Data management demands were underestimated. Treatment success was modest in all sectors (R=37.9%-72.0%) and did not align with treatment success reported by the state (6665/8770, 75.99%). One-fifth of TB providers (36/178, 20%) were doubtful that the low volume of patients with TB treated in their facility merited mastery of the extensive TB notification forms and procedures.
Conclusions: Subnational inventory studies can be rigorous, relevant, and efficient in countries that need them even in the absence of World Health Organization preconditions, if precautions are taken. The use of triangulation techniques, with minimal recourse to sampling and extrapolation, and the privileging of practical information needs of local decision makers yield reasonable misreporting estimates and viable policy recommendations.
Keywords: epidemiology; infectious disease notification; infectious disease reporting; integrated disease surveillance reporting; inventory study; notification; private sector; public health surveillance; tuberculosis.
©Ellen M H Mitchell, Olusola Adedeji Adejumo, Hussein Abdur-Razzaq, Chidubem Ogbudebe, Nkem Chukwueme, Samson Bamidele Olorunju, Mustapha Gidado. Originally published in JMIR Public Health and Surveillance (http://publichealth.jmir.org), 15.03.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
The Role of Trust as a Driver of Private-Provider Participation in Disease Surveillance: Cross-Sectional Survey From Nigeria.JMIR Public Health Surveill. 2024 Apr 25;10:e52191. doi: 10.2196/52191. JMIR Public Health Surveill. 2024. PMID: 38506095 Free PMC article.
-
From DOTS to the Stop TB Strategy: DOTS coverage and trend of tuberculosis notification in Ebonyi, southeastern Nigeria, 1998-2009.Pan Afr Med J. 2011;9:12. doi: 10.4314/pamj.v9i1.71187. Epub 2011 May 31. Pan Afr Med J. 2011. PMID: 22145056 Free PMC article.
-
Incomplete tuberculosis reporting and registration to the surveillance system in southwestern China of Yunnan Province: an inventory survey.BMC Public Health. 2024 May 25;24(1):1397. doi: 10.1186/s12889-024-18794-2. BMC Public Health. 2024. PMID: 38789991 Free PMC article.
-
Mandatory tuberculosis case notification in high tuberculosis-incidence countries: policy and practice.Eur Respir J. 2016 Dec;48(6):1571-1581. doi: 10.1183/13993003.00956-2016. Epub 2016 Oct 20. Eur Respir J. 2016. PMID: 27824601 Free PMC article. Review.
-
Epidemiology of tuberculosis in Papua New Guinea: analysis of case notification and treatment-outcome data, 2008-2016.Western Pac Surveill Response J. 2018 Jun 15;9(2):9-19. doi: 10.5365/wpsar.2018.9.1.006. eCollection 2018 Apr-Jun. Western Pac Surveill Response J. 2018. PMID: 30057853 Free PMC article. Review.
Cited by
-
Assessment of TB underreporting by level of reporting system in Lagos, Nigeria.Public Health Action. 2022 Sep 21;12(3):115-120. doi: 10.5588/pha.22.0008. Public Health Action. 2022. PMID: 36160719 Free PMC article.
-
Evaluation of Social and Clinical Factors Associated with Adverse Drug Reactions Among Children with Drug-Resistant Tuberculosis in Pakistan.Trop Med Infect Dis. 2025 Jun 20;10(7):176. doi: 10.3390/tropicalmed10070176. Trop Med Infect Dis. 2025. PMID: 40711054 Free PMC article.
-
The Role of Trust as a Driver of Private-Provider Participation in Disease Surveillance: Cross-Sectional Survey From Nigeria.JMIR Public Health Surveill. 2024 Apr 25;10:e52191. doi: 10.2196/52191. JMIR Public Health Surveill. 2024. PMID: 38506095 Free PMC article.
-
Tuberculosis case notifications and outcomes in Peruvian prisons prior to and during the COVID-19 pandemic: a national-level interrupted time series analysis.Lancet Reg Health Am. 2024 Mar 27;33:100723. doi: 10.1016/j.lana.2024.100723. eCollection 2024 May. Lancet Reg Health Am. 2024. PMID: 38800646 Free PMC article.
-
A Scoping Review on Accentuating the Pragmatism in the Implication of Mobile Health (mHealth) Technology for Tuberculosis Management in India.J Pers Med. 2022 Sep 28;12(10):1599. doi: 10.3390/jpm12101599. J Pers Med. 2022. PMID: 36294738 Free PMC article.
References
-
- Ansumana R, Keitell S, Roberts GM, Ntoumi F, Petersen E, Ippolito G, Zumla A. Impact of infectious disease epidemics on tuberculosis diagnostic, management, and prevention services: experiences and lessons from the 2014–2015 Ebola virus disease outbreak in West Africa. International Journal of Infectious Diseases. 2017 Mar;56:101–104. doi: 10.1016/j.ijid.2016.10.010. - DOI - PMC - PubMed
-
- World Health Organization . Assessing Tuberculosis Under-Reporting Through Inventory Studies. Switzerland: World Health Organization; 2012.
-
- Anyaehie U, Nwakoby B, Chikwendu C, Dim C, Uguru N, Oluka C, Ogugua C. Constraints, challenges and prospects of public-private partnership in health-care delivery in a developing economy. Ann Med Health Sci Res. 2014 Jan;4(1):61–6. doi: 10.4103/2141-9248.126615. http://www.amhsr.org/article.asp?issn=2141-9248;year=2014;volume=4;issue... - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
