

What was the Prevalence of COVID-19 in Asymptomatic Patients Undergoing Orthopaedic Surgery in One Large United States City Mid-pandemic?
- PMID: 33720056
- PMCID: PMC8277266
- DOI: 10.1097/CORR.0000000000001697
What was the Prevalence of COVID-19 in Asymptomatic Patients Undergoing Orthopaedic Surgery in One Large United States City Mid-pandemic?
Abstract
Background: Many patients with coronavirus disease 2019 (COVID-19) are asymptomatic. The prevalence of COVID-19 in orthopaedic populations will vary depending on the time and place where the sampling is performed. The idea that asymptomatic carriers play a role is generalizable but has not been studied in large populations of patients undergoing elective orthopaedic surgery. We therefore evaluated this topic in one large, metropolitan city in a state that had the ninth-most infections in the United States at the time this study was completed (June 2020). This work was based on a screening and testing protocol that required all patients to be tested for COVID-19 preoperatively.
Questions/purposes: (1) What is the prevalence of asymptomatic COVID-19 infection in patients planning to undergo orthopaedic surgery in one major city, in order to provide other surgeons with a framework for assessing COVID-19 rates in their healthcare system? (2) How did patients with positive test results for COVID-19 differ in terms of age, sex, and orthopaedic conditions? (3) What proportion of patients had complications treated, and how many patients had a symptomatic COVID-19 infection within 30 days of surgery (recognizing that some may have been missed and so our estimates of event rates will necessarily underestimate the frequency of this event)?
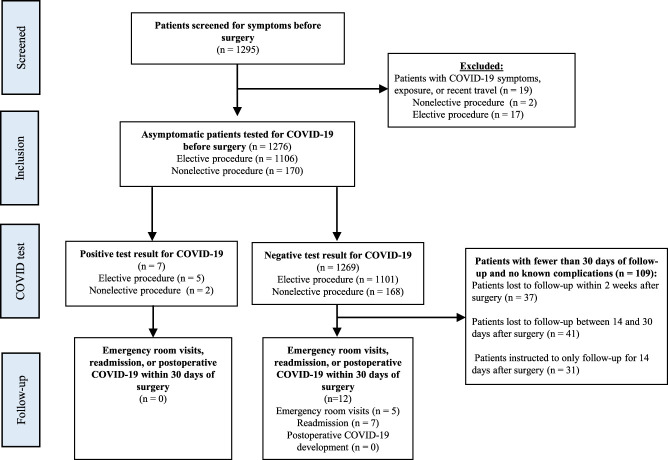
Methods: All adult patients scheduled for surgery at four facilities (two tertiary care hospitals, one orthopaedic specialty hospital, and one ambulatory surgery center) at a single institution in the Philadelphia metropolitan area from April 27, 2020 to June 12, 2020 were included in this study. A total of 1295 patients were screened for symptoms, exposure, temperature, and oxygen saturation via a standardized protocol before surgical scheduling; 1.5% (19 of 1295) were excluded because they had COVID-19 symptoms, exposure, or recent travel based on the initial screening questionnaire, leaving 98.5% (1276 of 1295) who underwent testing for COVID-19 preoperatively. All 1276 patients who passed the initial screening test underwent nasopharyngeal swabbing for COVID-19 via reverse transcription polymerase chain reaction before surgery. The mean age at the time of testing was 56 ± 16 years, and 53% (672 of 1276) were men. Eighty-seven percent (1106), 8% (103), and 5% (67) were tested via the Roche, Abbott, and Cepheid assays, respectively. All patients undergoing elective surgery were tested via the Roche assay, while those undergoing nonelective surgery received either the Abbott or Cepheid assay, based on availability. Patients with positive test results undergoing elective surgery had their procedures rescheduled, while patients scheduled for nonelective surgery underwent surgery regardless of their test results. Additionally, we reviewed the records of all patients at 30 days postoperatively for emergency room visits, readmissions, and COVID-19-related complications via electronic medical records and surgeon-reported complications. However, we had no method for definitively determining how many patients had complications, emergency department visits, or readmissions outside our system, so our event rate estimates for these endpoints are necessarily best-case estimates.
Results: A total of 0.5% (7 of 1276) of the patients tested positive for COVID-19: five via the Roche assay and two via the Abbott assay. Patients with positive test results were younger than those with negative results (39 ± 12 years versus 56 ± 16 years; p = 0.01). With the numbers available, we found no difference in the proportion of patients with positive test results for COVID-19 based on subspecialty area (examining the lowest and highest point estimates, respectively, we observed: trauma surgery [3%; 2 of 68 patients] versus hip and knee [0.3%; 1 of 401 patients], OR 12 [95% CI 1-135]; p = 0.06). No patients with negative preoperative test results for COVID-19 developed a symptomatic COVID-19 infection within 30 days postoperatively. Within 30 days of surgery, 0.9% (11 of 1276) of the patients presented to the emergency room, and 1.3% (16 of 1276) were readmitted for non-COVID-19-related complications. None of the patients with positive test results for COVID-19 preoperatively experienced complications. However, because some were likely treated outside our healthcare system, the actual percentages may be higher.
Conclusion: Because younger patients are more likely to be asymptomatic carriers of disease, surgeons should emphasize the importance of taking proper precautions to prevent virus exposure preoperatively. Because the rates of COVID-19 infection differ based on city and time, surgeons should monitor the local prevalence of disease to properly advise patients on the risk of COVID-19 exposure. Further investigation is required to assess the prevalence in the orthopaedic population in cities with larger COVID-19 burdens.
Level of evidence: Level III, therapeutic study.
Copyright © 2021 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that neither he nor she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: What was the Prevalence of COVID-19 in Asymptomatic Patients Undergoing Orthopaedic Surgery in One Large United States City Mid-pandemic?Clin Orthop Relat Res. 2021 Aug 1;479(8):1700-1702. doi: 10.1097/CORR.0000000000001755. Clin Orthop Relat Res. 2021. PMID: 33835094 Free PMC article. No abstract available.
Similar articles
-
Universal Testing for COVID-19 in Essential Orthopaedic Surgery Reveals a High Percentage of Asymptomatic Infections.J Bone Joint Surg Am. 2020 Aug 19;102(16):1379-1388. doi: 10.2106/JBJS.20.01053. J Bone Joint Surg Am. 2020. PMID: 32516279
-
Effectiveness and cost-effectiveness of four different strategies for SARS-CoV-2 surveillance in the general population (CoV-Surv Study): a structured summary of a study protocol for a cluster-randomised, two-factorial controlled trial.Trials. 2021 Jan 8;22(1):39. doi: 10.1186/s13063-020-04982-z. Trials. 2021. PMID: 33419461 Free PMC article.
-
Asymptomatic Pre-Operative COVID-19 Screening for Essential and Elective Surgeries: Early Results of Universal Screening at a Midwestern Academic Medical Center.Iowa Orthop J. 2021;41(1):33-38. Iowa Orthop J. 2021. PMID: 34552401 Free PMC article.
-
The theoretical mortality risk of an asymptomatic patient with a negative SARS-CoV-2 test developing COVID-19 following elective orthopaedic surgery.Bone Joint J. 2020 Sep;102-B(9):1256-1260. doi: 10.1302/0301-620X.102B9.BJJ-2020-1147.R1. Epub 2020 Jul 6. Bone Joint J. 2020. PMID: 32627569 Review.
-
Is There An Association Between Bundled Payments and "Cherry Picking" and "Lemon Dropping" in Orthopaedic Surgery? A Systematic Review.Clin Orthop Relat Res. 2021 Nov 1;479(11):2430-2443. doi: 10.1097/CORR.0000000000001792. Clin Orthop Relat Res. 2021. PMID: 33942797 Free PMC article.
Cited by
-
The Persistent Backlog of Knee and Shoulder Orthopedic Sport Surgery Case Volume Following the COVID-19 Pandemic.Arch Bone Jt Surg. 2023;11(12):738-751. doi: 10.22038/ABJS.2023.71724.3348. Arch Bone Jt Surg. 2023. PMID: 38146523 Free PMC article.
-
Results of COVID-19 screening in a dermatologic clinic in Northern Italy.J Prev Med Hyg. 2023 May 16;64(1):E1-E2. doi: 10.15167/2421-4248/jpmh2023.64.1.2544. eCollection 2023 Mar. J Prev Med Hyg. 2023. PMID: 37293464 Free PMC article. No abstract available.
-
No Patients Having Elective Outpatient Orthopaedic Surgery Performed in an Ambulatory Surgery Center Using Preoperative Screening Protocols During the Coronavirus Pandemic Developed COVID-19.Arthrosc Sports Med Rehabil. 2021 Aug;3(4):e1141-e1146. doi: 10.1016/j.asmr.2021.05.001. Epub 2021 May 12. Arthrosc Sports Med Rehabil. 2021. PMID: 34002168 Free PMC article.
-
Asymptomatic SARS-CoV-2 infection: A systematic review and meta-analysis.Proc Natl Acad Sci U S A. 2021 Aug 24;118(34):e2109229118. doi: 10.1073/pnas.2109229118. Proc Natl Acad Sci U S A. 2021. PMID: 34376550 Free PMC article.
References
-
- Balakrishnan K, Schechtman S, Hogikyan ND, Teoh AYB, McGrath B, Brenner MJ. COVID-19 pandemic: what every otolaryngologist–head and neck surgeon needs to know for safe airway management. Otolaryngol Head Neck Surg. 2020;162:804-808. - PubMed
-
- Blumberg TJ, Adler AC, Lin EE, et al. Universal screening for COVID-19 in children undergoing orthopaedic surgery: a multicenter report. J Pediatr Orthop . 2020;40:e990-e993. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
