

Models of supportive care in oncology
- PMID: 33720070
- PMCID: PMC8641044
- DOI: 10.1097/CCO.0000000000000733
Models of supportive care in oncology
Abstract
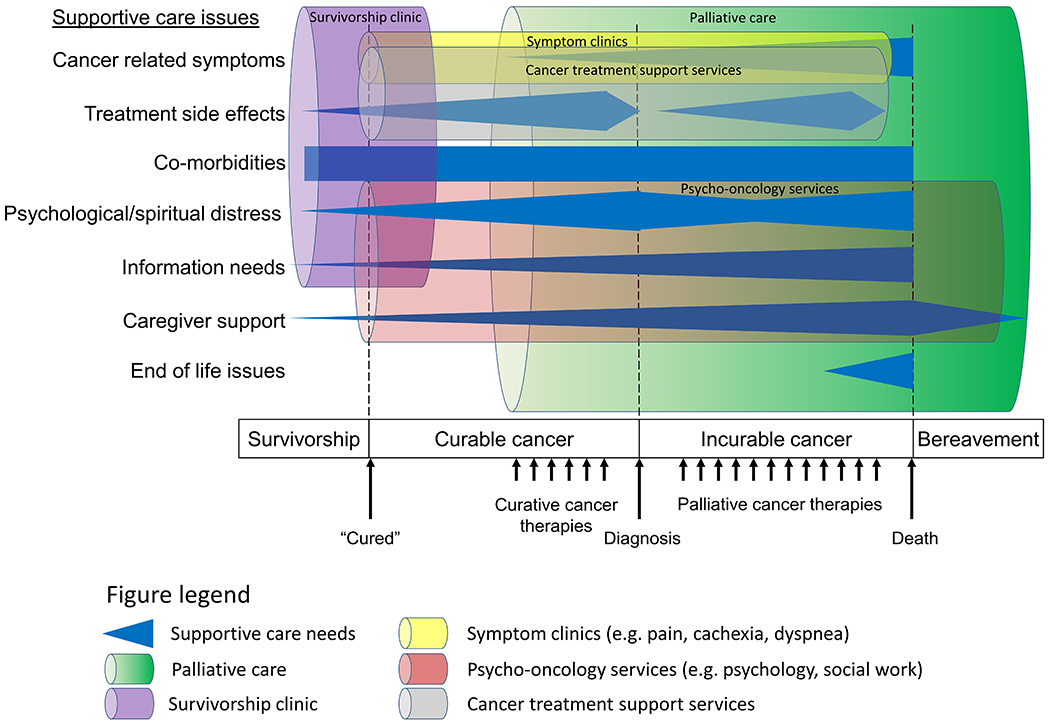
Purpose of review: Supportive care services have evolved overtime to meet the growing supportive care need of patients with cancer and their families. In this review, we summarize existing definitions of supportive care, highlight empiric studies on supportive care delivery, and propose an integrated conceptual framework on supportive cancer care.
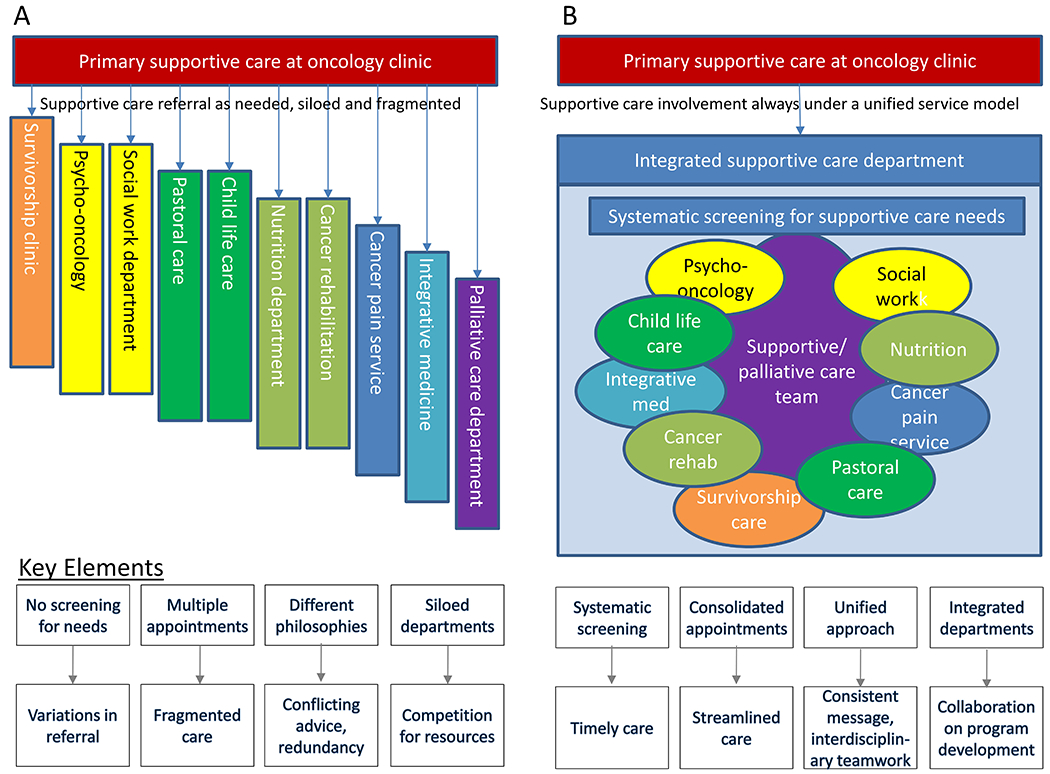
Recent findings: Supportive care aims at addressing the patients' physical, emotional, social, spiritual, and informational needs throughout the disease trajectory. Interdisciplinary teams are needed to deliver multidimensional care. Oncology teams have an important role providing supportive care in the front lines and referring patients to supportive care services such as palliative care, social work, rehabilitation, psycho-oncology, and integrative medicine. However, the current model of as needed referral and siloed departments can lead to heterogeneous access and fragmented care. To overcome these challenges, we propose a conceptual model in which supportive care services are organized under one department with a unified approach to patient care, program development, and research. Key features of this model include universal referral, systematic screening, tailored specialist involvement, streamlined care, collaborative teamwork, and enhanced outcomes.
Summary: Further research is needed to develop and test innovative supportive care models that can improve patient outcomes.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest:
None
Figures
References
-
- Hui D, Bruera E: Supportive and palliative oncology: A new paradigm for comprehensive cancer care. Hematology & Oncology Review 2013. 9:68–74.
-
- Chang VT, Hwang SS, Feuerman M et al. Symptom and quality of life survey of medical oncology patients at a veterans affairs medical center: A role for symptom assessment. Cancer 2000; 88:1175–1183. - PubMed
-
- Solano JP, Gomes B, Higginson IJ: A comparison of symptom prevalence in far advanced cancer, aids, heart disease, chronic obstructive pulmonary disease and renal disease. J Pain Symptom Manage 2006; 31:58–69. - PubMed
-
- Gray RE, Goel V, Fitch MI et al. Utilization of professional supportive care services by women with breast cancer. Breast Cancer Res Treat 2000; 64:253–258. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
