

Effect of Osteopathic Manipulative Treatment vs Sham Treatment on Activity Limitations in Patients With Nonspecific Subacute and Chronic Low Back Pain: A Randomized Clinical Trial
- PMID: 33720272
- PMCID: PMC7961471
- DOI: 10.1001/jamainternmed.2021.0005
Effect of Osteopathic Manipulative Treatment vs Sham Treatment on Activity Limitations in Patients With Nonspecific Subacute and Chronic Low Back Pain: A Randomized Clinical Trial
Abstract
Importance: Osteopathic manipulative treatment (OMT) is frequently offered to people with nonspecific low back pain (LBP) but never compared with sham OMT for reducing LBP-specific activity limitations.
Objective: To compare the efficacy of standard OMT vs sham OMT for reducing LBP-specific activity limitations at 3 months in persons with nonspecific subacute or chronic LBP.
Design, setting, and participants: This prospective, parallel-group, single-blind, single-center, sham-controlled randomized clinical trial recruited participants with nonspecific subacute or chronic LBP from a tertiary care center in France starting February 17, 2014, with follow-up completed on October 23, 2017. Participants were randomly allocated to interventions in a 1:1 ratio. Data were analyzed from March 22, 2018, to December 5, 2018.
Interventions: Six sessions (1 every 2 weeks) of standard OMT or sham OMT delivered by nonphysician, nonphysiotherapist osteopathic practitioners.
Main outcomes and measures: The primary end point was mean reduction in LBP-specific activity limitations at 3 months as measured by the self-administered Quebec Back Pain Disability Index (score range, 0-100). Secondary outcomes were mean reduction in LBP-specific activity limitations; mean changes in pain and health-related quality of life; number and duration of sick leaves, as well as number of LBP episodes at 12 months; and consumption of analgesics and nonsteroidal anti-inflammatory drugs at 3 and 12 months. Adverse events were self-reported at 3, 6, and 12 months.
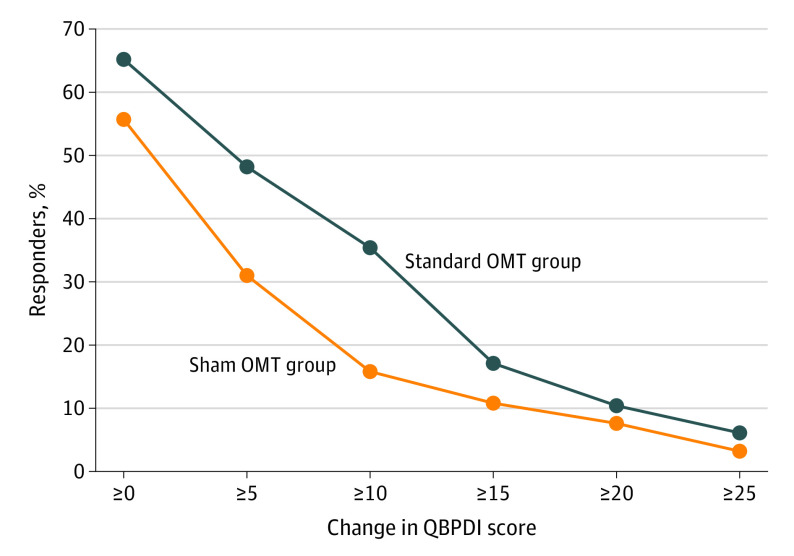
Results: Overall, 200 participants were randomly allocated to standard OMT and 200 to sham OMT, with 197 analyzed in each group; the median (range) age at inclusion was 49.8 (40.7-55.8) years, 235 of 394 (59.6%) participants were women, and 359 of 393 (91.3%) were currently working. The mean (SD) duration of the current LBP episode was 7.5 (14.2) months. Overall, 164 (83.2%) patients in the standard OMT group and 159 (80.7%) patients in the sham OMT group had the primary outcome data available at 3 months. The mean (SD) Quebec Back Pain Disability Index scores for the standard OMT group were 31.5 (14.1) at baseline and 25.3 (15.3) at 3 months, and in the sham OMT group were 27.2 (14.8) at baseline and 26.1 (15.1) at 3 months. The mean reduction in LBP-specific activity limitations at 3 months was -4.7 (95% CI, -6.6 to -2.8) and -1.3 (95% CI, -3.3 to 0.6) for the standard OMT and sham OMT groups, respectively (mean difference, -3.4; 95% CI, -6.0 to -0.7; P = .01). At 12 months, the mean difference in mean reduction in LBP-specific activity limitations was -4.3 (95% CI, -7.6 to -1.0; P = .01), and at 3 and 12 months, the mean difference in mean reduction in pain was -1.0 (95% CI, -5.5 to 3.5; P = .66) and -2.0 (95% CI, -7.2 to 3.3; P = .47), respectively. There were no statistically significant differences in other secondary outcomes. Four and 8 serious adverse events were self-reported in the standard OMT and sham OMT groups, respectively, though none was considered related to OMT.
Conclusions and relevance: In this randomized clinical trial of patients with nonspecific subacute or chronic LBP, standard OMT had a small effect on LBP-specific activity limitations vs sham OMT. However, the clinical relevance of this effect is questionable.
Trial registration: ClinicalTrials.gov Identifier: NCT02034864.
Conflict of interest statement
Figures

Comment in
-
Osteopathic Manipulative Treatment for Chronic Low Back Pain-Reply.JAMA Intern Med. 2021 Aug 1;181(8):1143-1144. doi: 10.1001/jamainternmed.2021.3186. JAMA Intern Med. 2021. PMID: 34180942 No abstract available.
-
Osteopathic Manipulative Treatment for Chronic Low Back Pain.JAMA Intern Med. 2021 Aug 1;181(8):1143. doi: 10.1001/jamainternmed.2021.3183. JAMA Intern Med. 2021. PMID: 34180946 No abstract available.
-
Osteopathic Manipulative Treatment for Chronic Low Back Pain.JAMA Intern Med. 2021 Aug 1;181(8):1142-1143. doi: 10.1001/jamainternmed.2021.3180. JAMA Intern Med. 2021. PMID: 34180952 No abstract available.
References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789-1858. doi: 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- Qaseem A, Wilt TJ, McLean RM, Forciea MA; Clinical Guidelines Committee of the American College of Physicians . Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514-530. doi: 10.7326/M16-2367 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
