

Case-Control Study of Individuals with Discrepant Nucleocapsid and Spike Protein SARS-CoV-2 IgG Results
- PMID: 33720347
- PMCID: PMC7989591
- DOI: 10.1093/clinchem/hvab045
Case-Control Study of Individuals with Discrepant Nucleocapsid and Spike Protein SARS-CoV-2 IgG Results
Abstract
Background: Laboratory-based methods for SARS-CoV-2 antibody detection vary widely in performance. However, there are limited prospectively-collected data on assay performance, and minimal clinical information to guide interpretation of discrepant results.
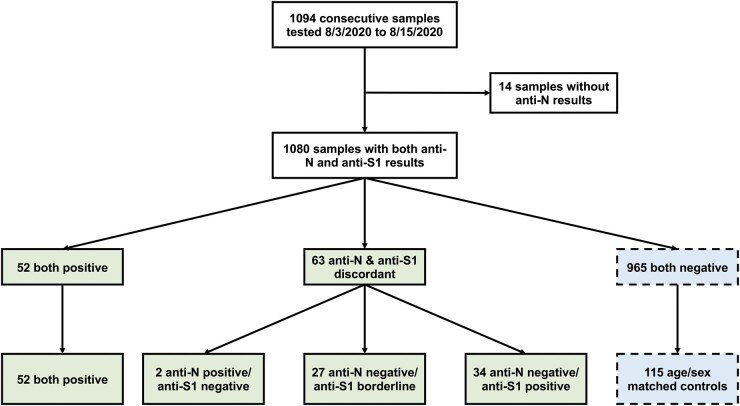
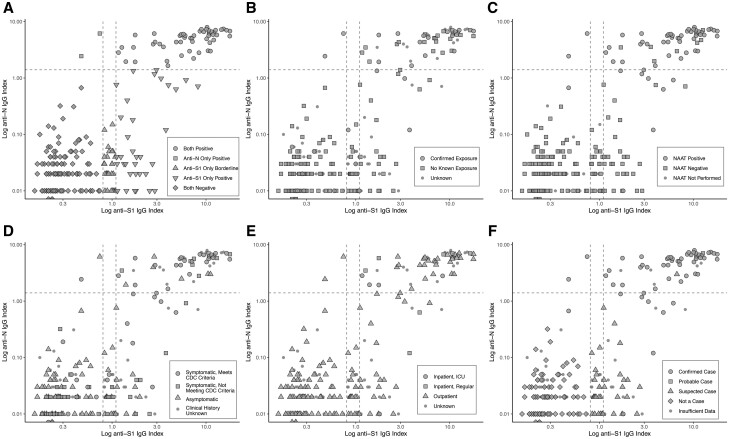
Methods: Over a 2-week period, 1080 consecutive plasma samples submitted for clinical SARS-CoV-2 IgG testing were tested in parallel for anti-nucleocapsid IgG (anti-N, Abbott) and anti-spike IgG (anti-S1, EUROIMMUN). Chart review was conducted for samples testing positive or borderline on either assay, and for an age/sex-matched cohort of samples negative by both assays. CDC surveillance case definitions were used to determine clinical sensitivity/specificity and conduct receiver operating characteristics curve analysis.
Results: There were 52 samples positive by both methods, 2 positive for anti-N only, 34 positive for anti-S1 only, and 27 borderline for anti-S1. Of the 34 individuals positive for anti-S1 alone, 8 (24%) had confirmed COVID-19. No anti-S1 borderline cases were positive for anti-N or had confirmed/probable COVID-19. The anti-N assay was less sensitive (84.2% [95% CI 72.1-92.5%] vs 94.7% [95% CI 85.4-98.9%]) but more specific (99.2% [95% CI 95.5-100%] vs 86.9% [95% CI 79.6-92.3%]) than anti-S1. Abbott anti-N sensitivity could be improved to 96.5% with minimal effect on specificity if the index threshold was lowered from 1.4 to 0.6.
Conclusion: Real-world concordance between different serologic assays may be lower than previously described in retrospective studies. These findings have implications for the interpretation of SARS-CoV-2 IgG results, especially with the advent of spike antigen-targeted vaccination, as a subset of patients with true infection are anti-N negative and anti-S1 positive.
Keywords: COVID-19; SARS-CoV-2; serology.
© American Association for Clinical Chemistry 2021.
Figures

Comment in
-
SARS-CoV-2 Serologic Testing: Facts, Fiction, and Fallacies.Clin Chem. 2021 Jul 6;67(7):924-926. doi: 10.1093/clinchem/hvab072. Clin Chem. 2021. PMID: 34077511 Free PMC article. No abstract available.
References
-
- Long Q-X, Liu B-Z, Deng H-J, Wu G-C, Deng K, Chen Y-K, et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat Med 2020;26:845–8. - PubMed
-
- Voysey M, Clemens SAC, Madhi SA, Weckx LY, Folegatti PM, Aley PK, et al. ; Oxford COVID Vaccine Trial Group. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021;397:99–111. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
