

Association of Clinical, Biological, and Brain Magnetic Resonance Imaging Findings With Electroencephalographic Findings for Patients With COVID-19
- PMID: 33720371
- PMCID: PMC7961310
- DOI: 10.1001/jamanetworkopen.2021.1489
Association of Clinical, Biological, and Brain Magnetic Resonance Imaging Findings With Electroencephalographic Findings for Patients With COVID-19
Erratum in
-
Group Members Added to Supplement.JAMA Netw Open. 2022 Jun 1;5(6):e2219899. doi: 10.1001/jamanetworkopen.2022.19899. JAMA Netw Open. 2022. PMID: 35708695 Free PMC article. No abstract available.
Abstract
Importance: There is evidence of central nervous system impairments associated with coronavirus disease 2019 (COVID-19) infection, including encephalopathy. Multimodal monitoring of patients with COVID-19 may delineate the specific features of COVID-19-related encephalopathy and guide clinical management.
Objectives: To investigate clinical, biological, and brain magnetic resonance imaging (MRI) findings in association with electroencephalographic (EEG) features for patients with COVID-19, and to better refine the features of COVID-19-related encephalopathy.
Design, setting, and participants: This retrospective cohort study conducted in Pitié-Salpêtrière Hospital, Paris, France, enrolled 78 hospitalized adults who received a diagnosis of severe acute respiratory syndrome coronavirus 2 (SARS-Cov2) and underwent EEG between March 30 and June 11, 2020.
Exposures: Detection of SARS-CoV-2 from a nasopharyngeal specimen using a reverse transcription-polymerase chain reaction assay or, in the case of associated pneumonia, on a computed tomography scan of the chest.
Main outcomes and measures: Data on the clinical and paraclinical features of the 78 patients with COVID-19 were retrieved from electronic patient records.
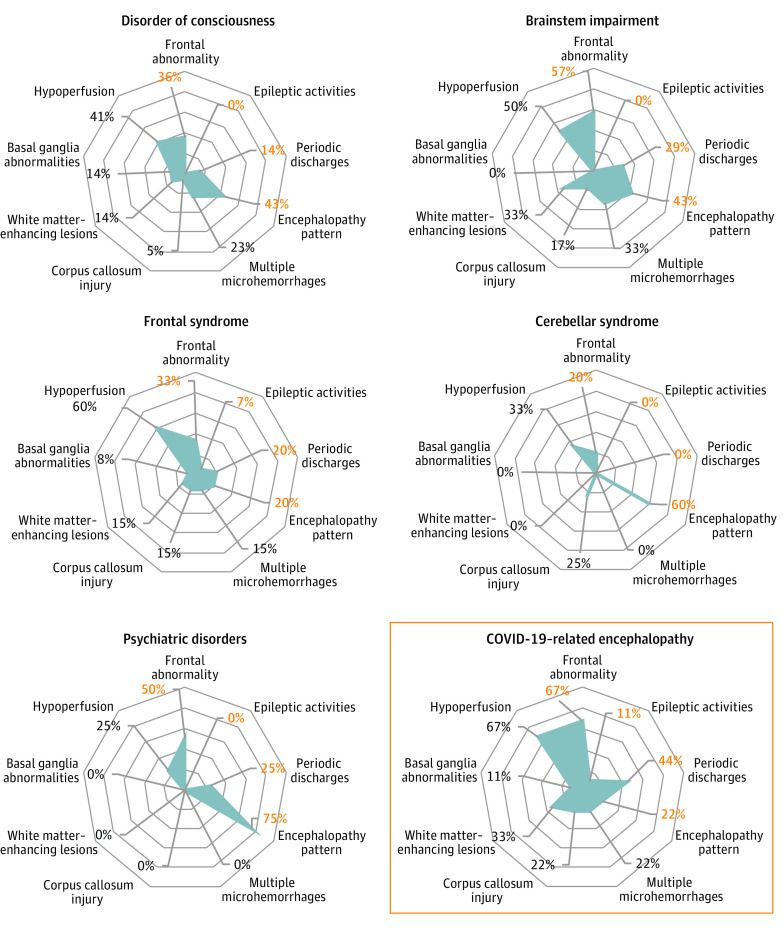
Results: Of 644 patients who were hospitalized for COVID-19, 78 (57 men [73%]; mean [SD] age, 61 [12] years) underwent EEG. The main indications for EEG were delirium, seizure-like events, and delayed awakening in the intensive care unit after stopping treatment with sedatives. Sixty-nine patients showed pathologic EEG findings, including metabolic-toxic encephalopathy features, frontal abnormalities, periodic discharges, and epileptic activities. Of 57 patients who underwent brain MRI, 41 showed abnormalities, including perfusion abnormalities, acute ischemic lesions, multiple microhemorrhages, and white matter-enhancing lesions. Fifty-five patients showed biological abnormalities, including dysnatremia, kidney failure, and liver dysfunction, the same day as the EEG. The results of cerebrospinal fluid analysis were negative for SARS-Cov-2 for all tested patients. Nine patients who had no identifiable cause of brain injury outside COVID-19 were further isolated; their brain injury was defined as COVID-19-related encephalopathy. They represented 1% (9 of 644) of patients with COVID-19 requiring hospitalization. Six of these 9 patients had movement disorders, 7 had frontal syndrome, 4 had brainstem impairment, 4 had periodic EEG discharges, and 3 had MRI white matter-enhancing lesions.
Conclusions and relevance: The results from this cohort of patients hospitalized with COVID-19 suggest there are clinical, EEG, and MRI patterns that could delineate specific COVID-19-related encephalopathy and guide treatment strategy.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
