

A majority of uninfected adults show preexisting antibody reactivity against SARS-CoV-2
- PMID: 33720905
- PMCID: PMC8119195
- DOI: 10.1172/jci.insight.146316
A majority of uninfected adults show preexisting antibody reactivity against SARS-CoV-2
Abstract
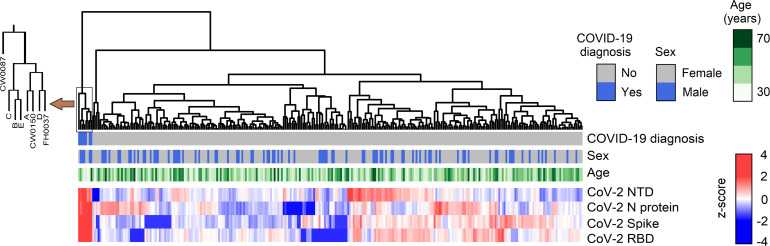
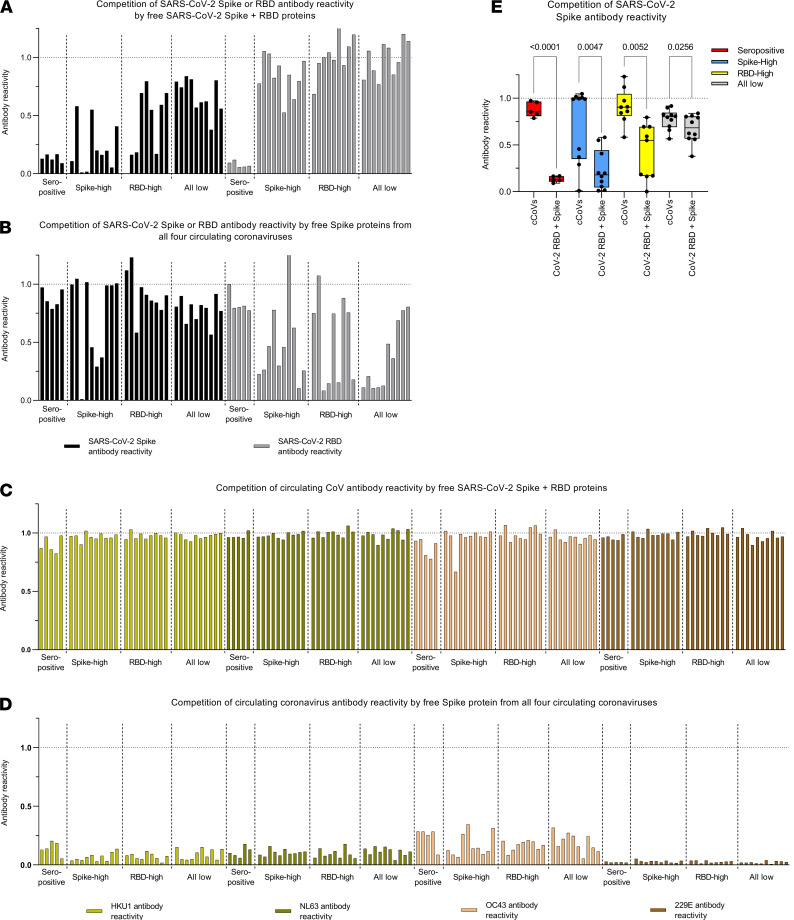
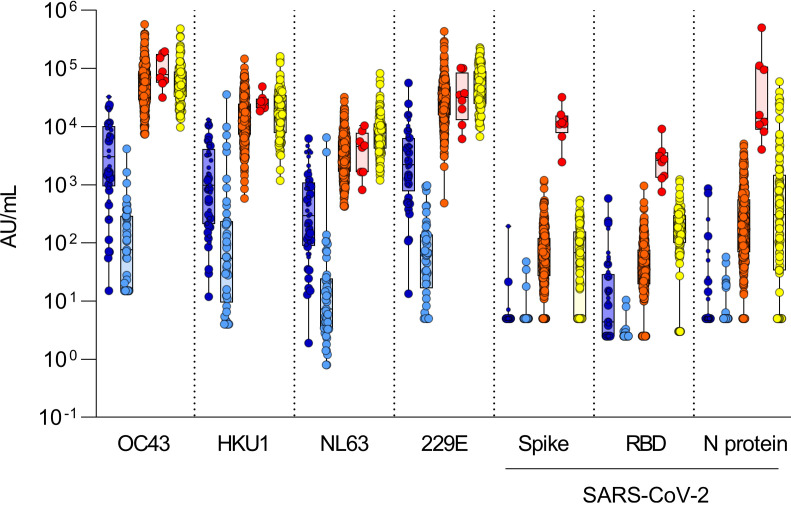
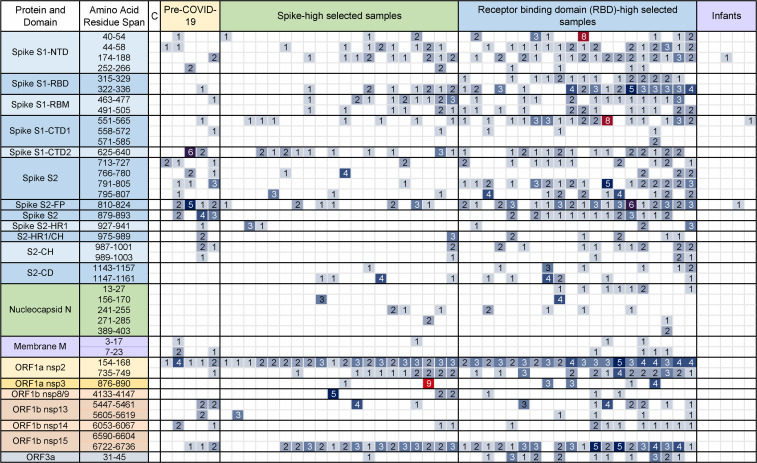
Preexisting cross-reactivity to SARS-CoV-2 occurs in the absence of prior viral exposure. However, this has been difficult to quantify at the population level due to a lack of reliably defined seroreactivity thresholds. Using an orthogonal antibody testing approach, we estimated that about 0.6% of nontriaged adults from the greater Vancouver, Canada, area between May 17 and June 19, 2020, showed clear evidence of a prior SARS-CoV-2 infection, after adjusting for false-positive and false-negative test results. Using a highly sensitive multiplex assay and positive/negative thresholds established in infants in whom maternal antibodies have waned, we determined that more than 90% of uninfected adults showed antibody reactivity against the spike protein, receptor-binding domain (RBD), N-terminal domain (NTD), or the nucleocapsid (N) protein from SARS-CoV-2. This seroreactivity was evenly distributed across age and sex, correlated with circulating coronaviruses' reactivity, and was partially outcompeted by soluble circulating coronaviruses' spike. Using a custom SARS-CoV-2 peptide mapping array, we found that this antibody reactivity broadly mapped to spike and to conserved nonstructural viral proteins. We conclude that most adults display preexisting antibody cross-reactivity against SARS-CoV-2, which further supports investigation of how this may impact the clinical severity of COVID-19 or SARS-CoV-2 vaccine responses.
Keywords: Adaptive immunity; COVID-19; Immunology.
Conflict of interest statement
Figures
Similar articles
-
Evaluation of a multiplexed coronavirus antigen array for detection of SARS-CoV-2 specific IgG in COVID-19 convalescent plasma.J Immunol Methods. 2021 Oct;497:113104. doi: 10.1016/j.jim.2021.113104. Epub 2021 Jul 22. J Immunol Methods. 2021. PMID: 34303688 Free PMC article.
-
Robust validation and performance comparison of immunogenicity assays assessing IgG and neutralizing antibodies to SARS-CoV-2.PLoS One. 2022 Feb 7;17(2):e0262922. doi: 10.1371/journal.pone.0262922. eCollection 2022. PLoS One. 2022. PMID: 35130298 Free PMC article.
-
Analysis of Serological Biomarkers of SARS-CoV-2 Infection in Convalescent Samples From Severe, Moderate and Mild COVID-19 Cases.Front Immunol. 2021 Nov 19;12:748291. doi: 10.3389/fimmu.2021.748291. eCollection 2021. Front Immunol. 2021. PMID: 34867975 Free PMC article.
-
Immunologic Testing for SARS-CoV-2 Infection from the Antigen Perspective.J Clin Microbiol. 2021 Apr 20;59(5):e02160-20. doi: 10.1128/JCM.02160-20. Print 2021 Apr 20. J Clin Microbiol. 2021. PMID: 33318065 Free PMC article. Review.
-
How to interpret and use COVID-19 serology and immunology tests.Clin Microbiol Infect. 2021 Jul;27(7):981-986. doi: 10.1016/j.cmi.2021.05.001. Epub 2021 May 8. Clin Microbiol Infect. 2021. PMID: 33975005 Free PMC article. Review.
Cited by
-
Enhanced Assessment of Cross-Reactive Antigenic Determinants within the Spike Protein.Int J Mol Sci. 2024 Jul 26;25(15):8180. doi: 10.3390/ijms25158180. Int J Mol Sci. 2024. PMID: 39125749 Free PMC article.
-
Pre-existing anti-HCoV-OC43 immunity influences the durability and cross-reactivity of humoral response to SARS-CoV-2 vaccination.Front Cell Infect Microbiol. 2022 Sep 2;12:978440. doi: 10.3389/fcimb.2022.978440. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36118022 Free PMC article.
-
SARS-CoV-2-The Role of Natural Immunity: A Narrative Review.J Clin Med. 2022 Oct 25;11(21):6272. doi: 10.3390/jcm11216272. J Clin Med. 2022. PMID: 36362500 Free PMC article. Review.
-
Seroconversion following COVID-19 vaccination: can we optimize protective response in CD20-treated individuals?Clin Exp Immunol. 2022 May 12;207(3):263-271. doi: 10.1093/cei/uxab015. Clin Exp Immunol. 2022. PMID: 35553629 Free PMC article.
-
Seasonal coronaviruses and SARS-CoV-2: effects of preexisting immunity during the COVID-19 pandemic.J Zhejiang Univ Sci B. 2022 Jun 15;23(6):451-460. doi: 10.1631/jzus.B2200049. J Zhejiang Univ Sci B. 2022. PMID: 35686525 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
