

Efficacy and Safety of Anti-TNFα Therapy for Uveitis Associated with Juvenile Idiopathic Arthritis: A Systematic Review and Meta-Analysis
- PMID: 33721267
- PMCID: PMC8217376
- DOI: 10.1007/s40744-021-00296-x
Efficacy and Safety of Anti-TNFα Therapy for Uveitis Associated with Juvenile Idiopathic Arthritis: A Systematic Review and Meta-Analysis
Abstract
Introduction: To investigate the efficacy and safety of anti-TNFα therapy in patients with juvenile idiopathic arthritis associated uveitis (JIA-U).
Methods: Embase, PubMed, Cochrane Library, and Web of Science were systematically searched for studies reporting anti-TNFα treatment in patients with JIA-U. The primary outcome was the control of intraocular inflammation (CII). The pooled proportion of CII was assessed by the random-effects method when I2 > 50%, otherwise, by the fixed-effect method. This study was registered with PROSPERO (CRD42020161749).
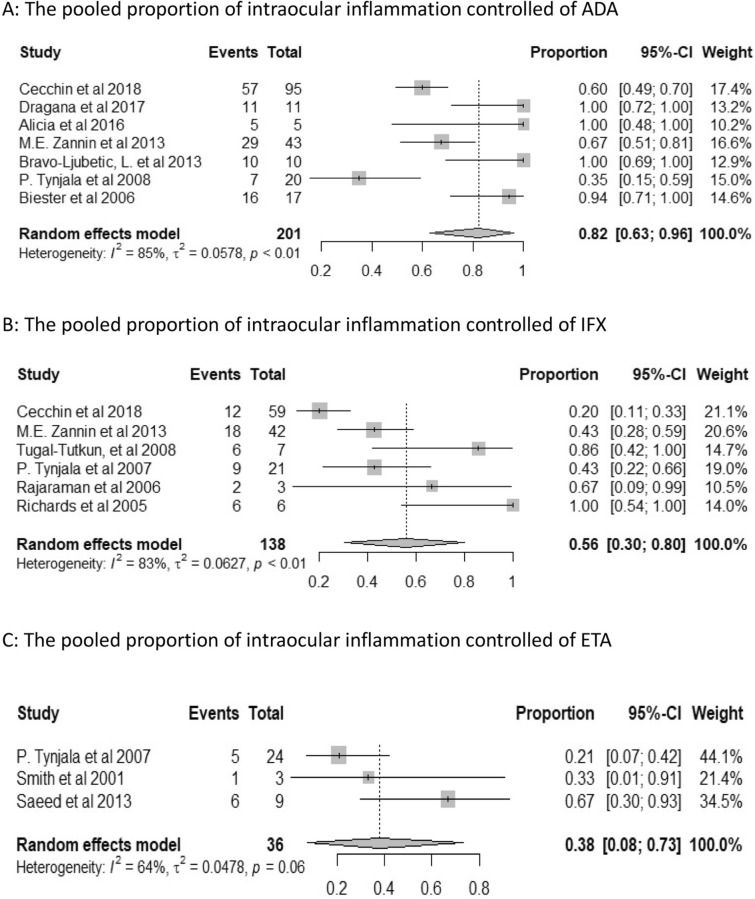
Results: Three randomized clinical trials (RCTs), twelve case series, three retrospective cohort studies, and three case reports were identified. A total of 399 patients were receiving anti-TNFα therapy, of which 201 patients were treated with adalimumab (ADA), 139 with infliximab (IFX), 36 with etanercept (ETA), 20 with golimumab (GLM), and 3 with certolizumab pegol (CZP). The pooled proportions of CII on observational studies were 82% (95% CI 63-96%) in patients receiving ADA, 56% (95% CI 30-80%) in IFX, 38% (95% CI 8-73%) in ETA and 65% (95% CI 42-86%) in GLM, respectively. All three patients treated with CZP reached improved activity. ADA therapy led to a significantly higher proportion of CII compared to IFX therapy (χ2 = 26.24, P < 0.001), or to ETA therapy (χ2 = 13.43, P < 0.001); but no statistical difference was observed between IFX and ETA (χ2 = 0.13, P = 0.71). As to safety, most reported adverse events were tolerable and two cohort studies consistently showed that ADA was safer than IFX.
Conclusions: The existing evidence suggests that ADA is better than IFX regarding efficacy and safety. The effectiveness of IFX is higher than ETA with no statistical difference. GLM and CZP may be proxies for ADA but the evidence is limited.
Keywords: Anti-TNFα therapy; Efficacy; Juvenile idiopathic arthritis; Meta-analysis.
Figures


References
-
- Heiligenhaus A, Heinz C, Edelsten C, Kotaniemi K, Minden K. Review for disease of the year: epidemiology of juvenile idiopathic arthritis and its associated uveitis: the probable risk factors. Ocul Immunol Inflamm. 2013;21(3):180–191. - PubMed
-
- Heiligenhaus A, Niewerth M, Ganser G, Heinz C, Minden K. Prevalence and complications of uveitis in juvenile idiopathic arthritis in a population-based nation-wide study in Germany: suggested modification of the current screening guidelines. Rheumatology (Oxford) 2007;46(6):1015–1019. - PubMed
-
- Tay-Kearney ML, Schwam BL, Lowder C, Dunn JP, Meisler DM, Vitale S, et al. Clinical features and associated systemic diseases of HLA-B27 uveitis. Am J Ophthalmol. 1996;121(1):47–56. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
