

Fetal body MRI and its application to fetal and neonatal treatment: an illustrative review
- PMID: 33721554
- PMCID: PMC7614154
- DOI: 10.1016/S2352-4642(20)30313-8
Fetal body MRI and its application to fetal and neonatal treatment: an illustrative review
Abstract
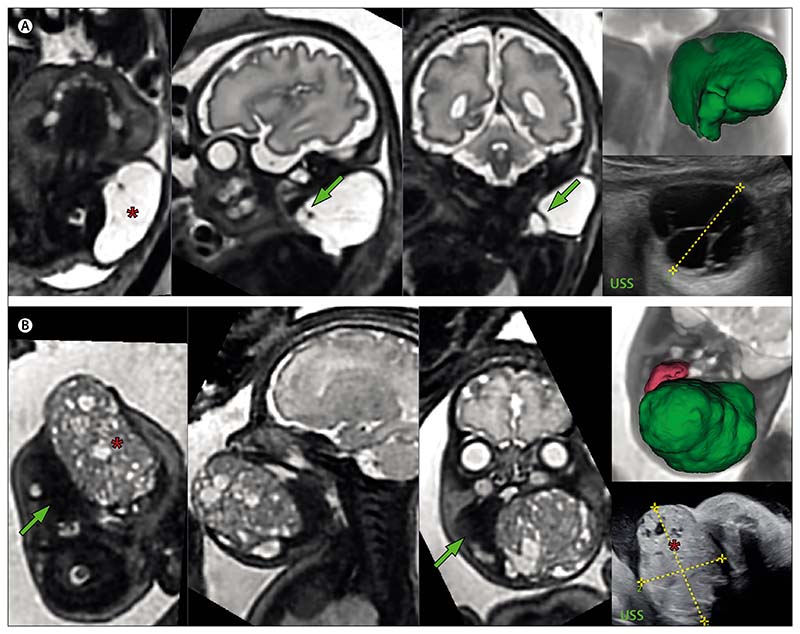
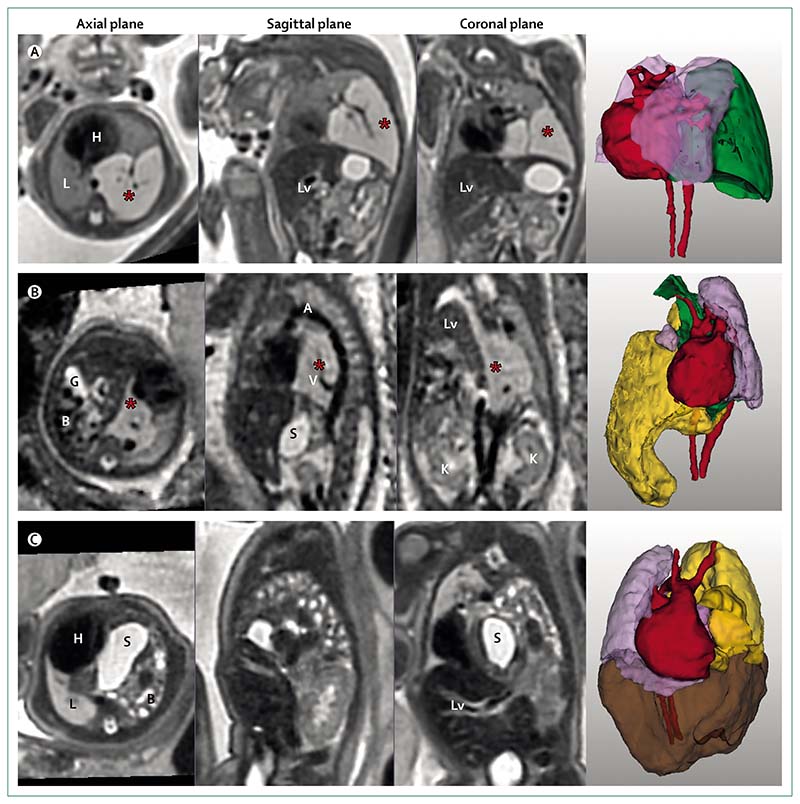
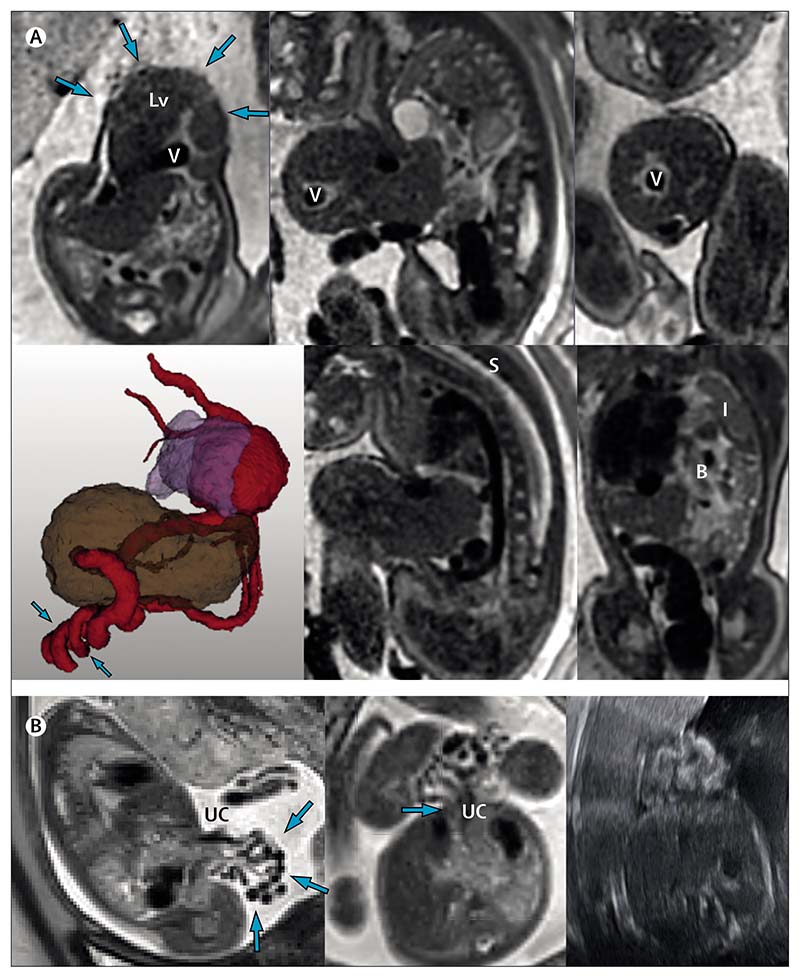
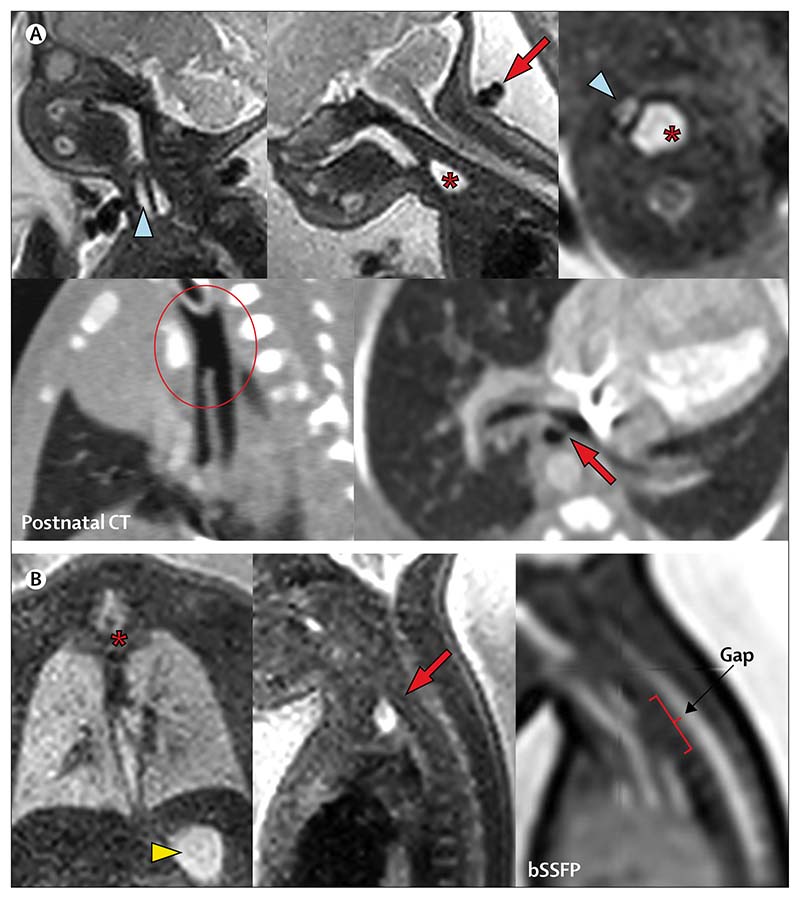
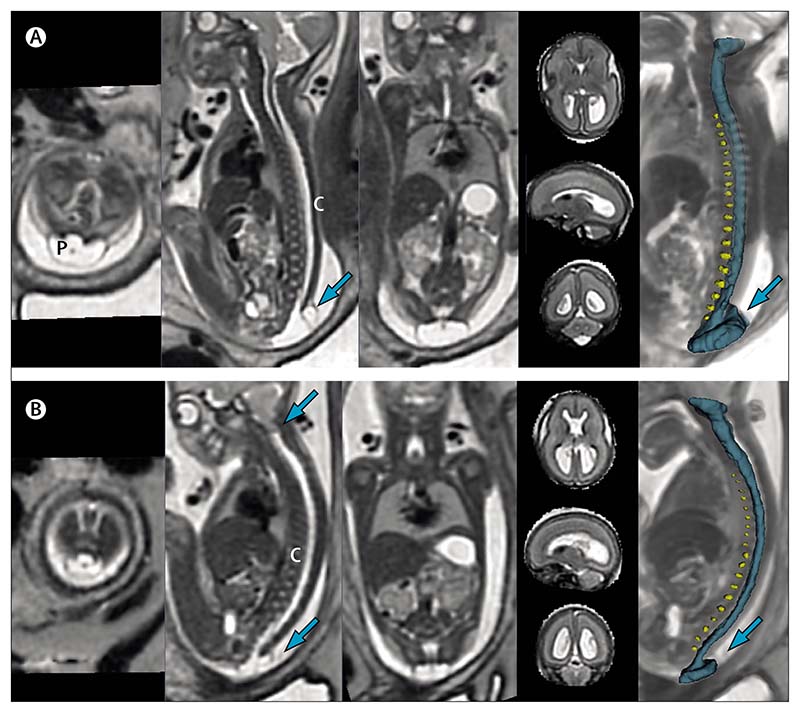
This Review depicts the evolving role of MRI in the diagnosis and prognostication of anomalies of the fetal body, here including head and neck, thorax, abdomen and spine. A review of the current literature on the latest developments in antenatal imaging for diagnosis and prognostication of congenital anomalies is coupled with illustrative cases in true radiological planes with viewable three-dimensional video models that show the potential of post-acquisition reconstruction protocols. We discuss the benefits and limitations of fetal MRI, from anomaly detection, to classification and prognostication, and defines the role of imaging in the decision to proceed to fetal intervention, across the breadth of included conditions. We also consider the current capabilities of ultrasound and explore how MRI and ultrasound can complement each other in the future of fetal imaging.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
JRD and AD declare grants from the Wellcome Trust and Engineering and Physical Sciences Research Council (EPSRC; GIFT-Surg Project). PDC is supported by a UK National Institute for Health Research (NIHR) professorship. MD declares grants from the Wellcome Trust, EPSRC, and NIHR. Other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
