

Midazolam Premedication Immediately Before Surgery Is Not Associated With Early Postoperative Delirium
- PMID: 33721875
- PMCID: PMC8373629
- DOI: 10.1213/ANE.0000000000005482
Midazolam Premedication Immediately Before Surgery Is Not Associated With Early Postoperative Delirium
Abstract
Background: Postoperative delirium is common among older surgical patients and may be associated with anesthetic management during the perioperative period. The aim of this study is to assess whether intravenous midazolam, a short-acting benzodiazepine used frequently as premedication, increased the incidence of postoperative delirium.
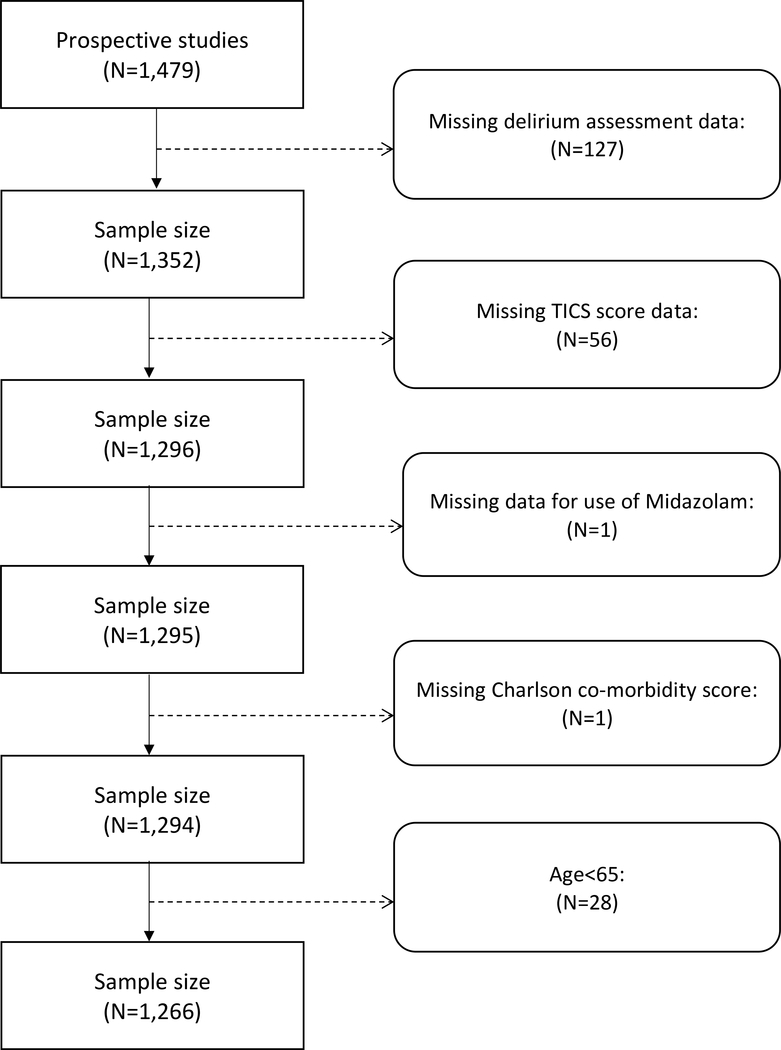
Methods: Analyses of existing data were conducted using a database created from 3 prospective studies in patients aged 65 years or older who underwent elective major noncardiac surgery. Postoperative delirium occurring on the first postoperative day was measured using the confusion assessment method. We assessed the association between the use or nonuse of premedication with midazolam and postoperative delirium using a χ2 test, using propensity scores to match up with 3 midazolam patients for each control patient who did not receive midazolam.
Results: A total of 1266 patients were included in this study. Intravenous midazolam was administered as premedication in 909 patients (72%), and 357 patients did not receive midazolam. Those who did and did not receive midazolam significantly differed in age, Charlson comorbidity scores, preoperative cognitive status, preoperative use of benzodiazepines, type of surgery, and year of surgery. Propensity score matching for these variables and American Society of Anesthesiology physical status scores resulted in propensity score-matched samples with 1-3 patients who used midazolam (N = 749) for each patient who did not receive midazolam (N = 357). After propensity score matching, all standardized differences in preoperative patient characteristics ranged from -0.07 to 0.06, indicating good balance on baseline variables between the 2 exposure groups. No association was found between premedication with midazolam and incident delirium on the morning of the first postoperative day in the matched dataset, with odds ratio (95% confidence interval) of 0.91 (0.65-1.29), P = .67.
Conclusions: Premedication using midazolam was not associated with higher incidence of delirium on the first postoperative day in older patients undergoing major noncardiac surgery.
Trial registration: ClinicalTrials.gov NCT03928236 NCT03052660.
Copyright © 2021 International Anesthesia Research Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Santana Santos F, Wahlund LO, Varli F, et al.Incidence, clinical features and subtypes of delirium in elderly patients treated for hip fractures. Dement Geriatr Cogn Disord. 2005;20:231–237. - PubMed
-
- Kalisvaart KJ, Vreeswijk R, de Jonghe JF, et al.Risk factors and prediction of postoperative delirium in elderly hip-surgery patients: implementation and validation of a medical risk factor model. J Am Geriatr Soc. 2006;54:817–822. - PubMed
-
- Lipowski ZJ. Delirium in the elderly patient. N Engl J Med. 1989;320:578–582. - PubMed
-
- Thomas RI, Cameron DJ, Fahs MC. A prospective study of delirium and prolonged hospital stay. Exploratory study. Arch Gen Psychiatry. 1988;45:937–940. - PubMed
-
- Marcantonio ER, Juarez G, Goldman L, et al.The relationship of postoperative delirium with psychoactive medications. JAMA. 1994;272:1518–1522. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
