

Tobacco Smoking and Risk of Second Primary Lung Cancer
- PMID: 33722709
- PMCID: PMC8159872
- DOI: 10.1016/j.jtho.2021.02.024
Tobacco Smoking and Risk of Second Primary Lung Cancer
Abstract
Introduction: Lung cancer survivors are at high risk of developing a second primary lung cancer (SPLC). However, SPLC risk factors have not been established and the impact of tobacco smoking remains controversial. We examined the risk factors for SPLC across multiple epidemiologic cohorts and evaluated the impact of smoking cessation on reducing SPLC risk.
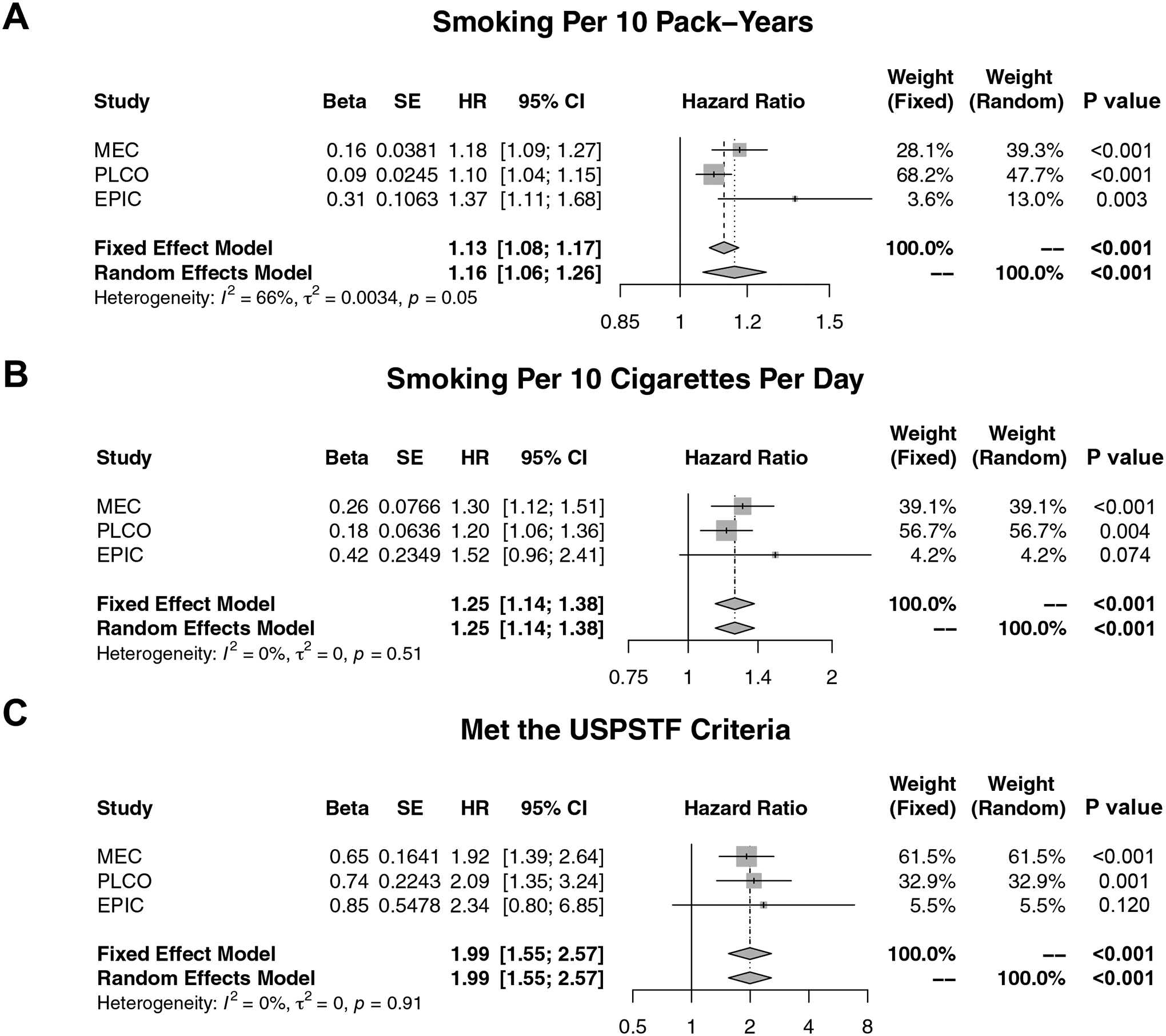
Methods: We analyzed data from 7059 participants in the Multiethnic Cohort (MEC) diagnosed with an initial primary lung cancer (IPLC) between 1993 and 2017. Cause-specific proportional hazards models estimated SPLC risk. We conducted validation studies using the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial (N = 3423 IPLC cases) and European Prospective Investigation into Cancer and Nutrition (N = 4731 IPLC cases) cohorts and pooled the SPLC risk estimates using random effects meta-analysis.
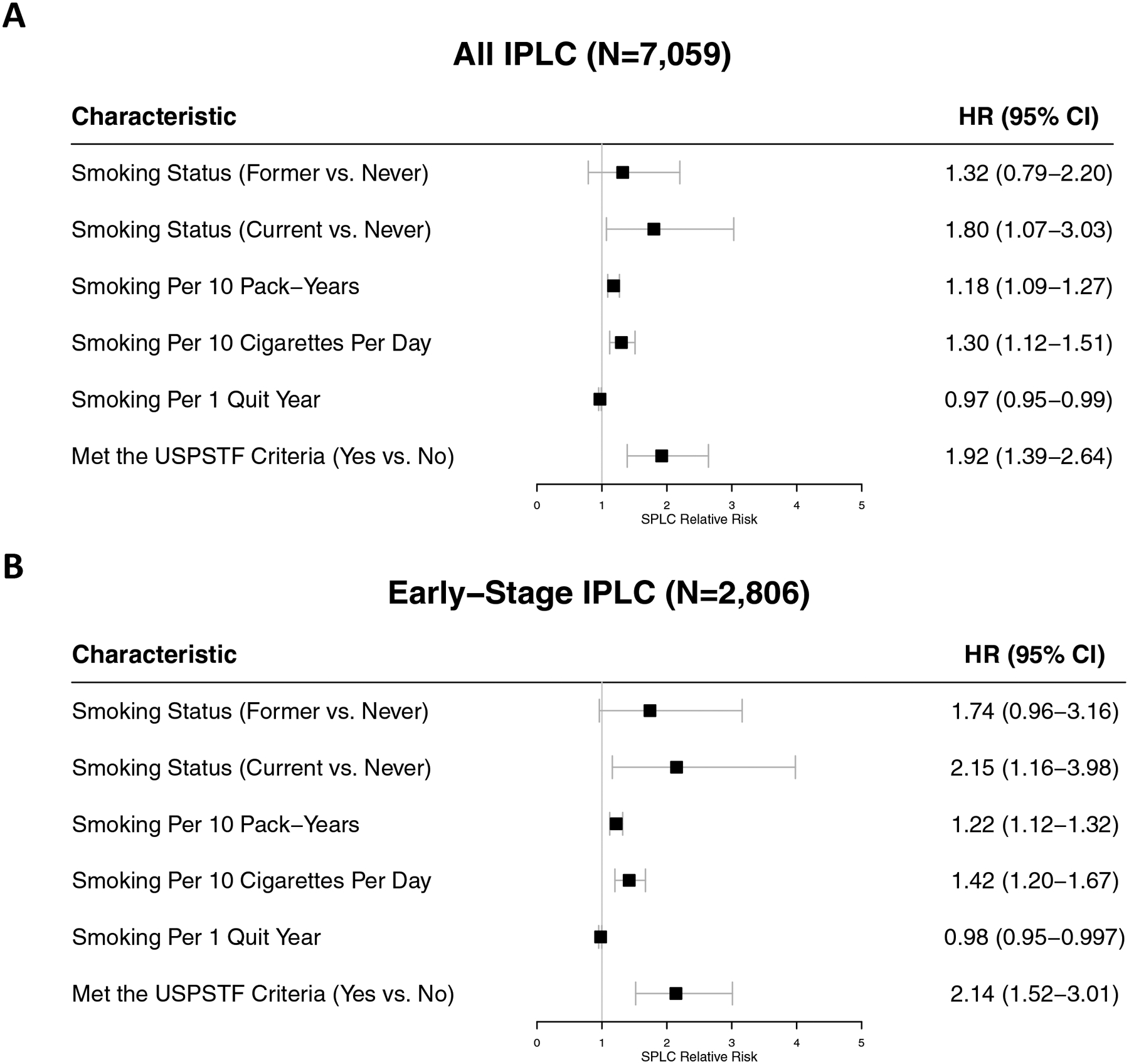
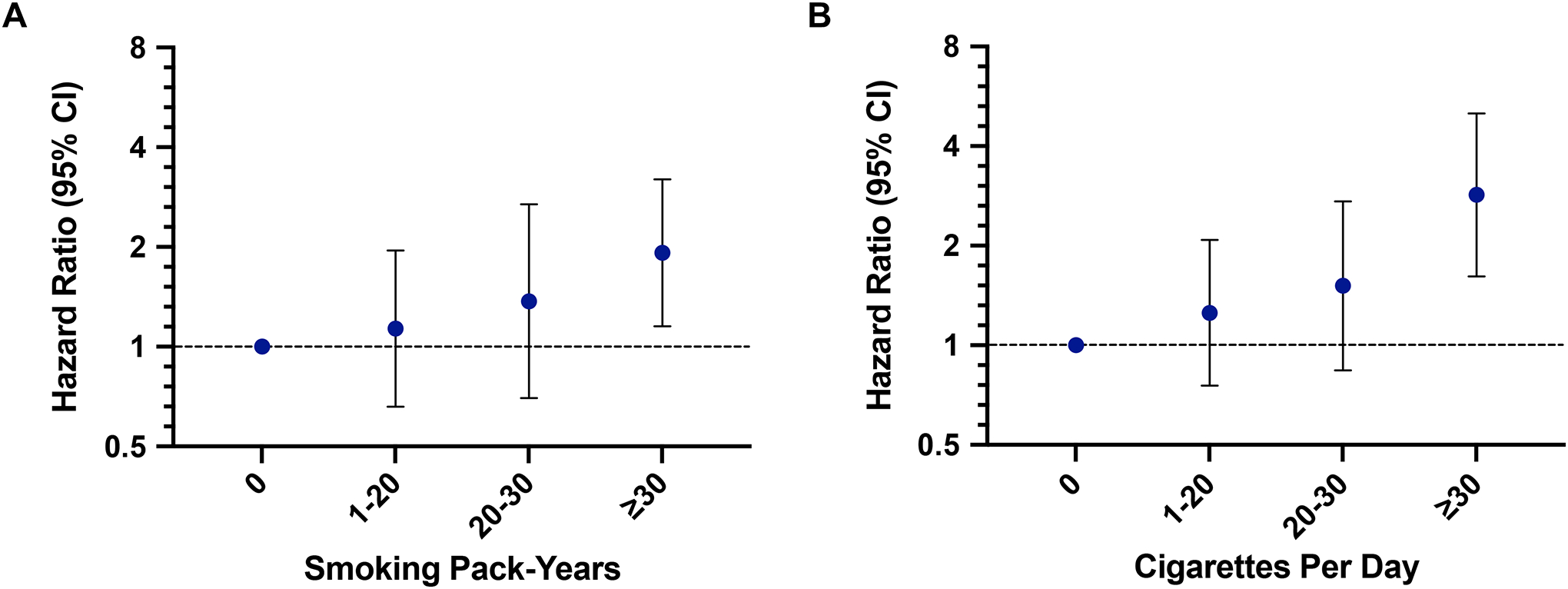
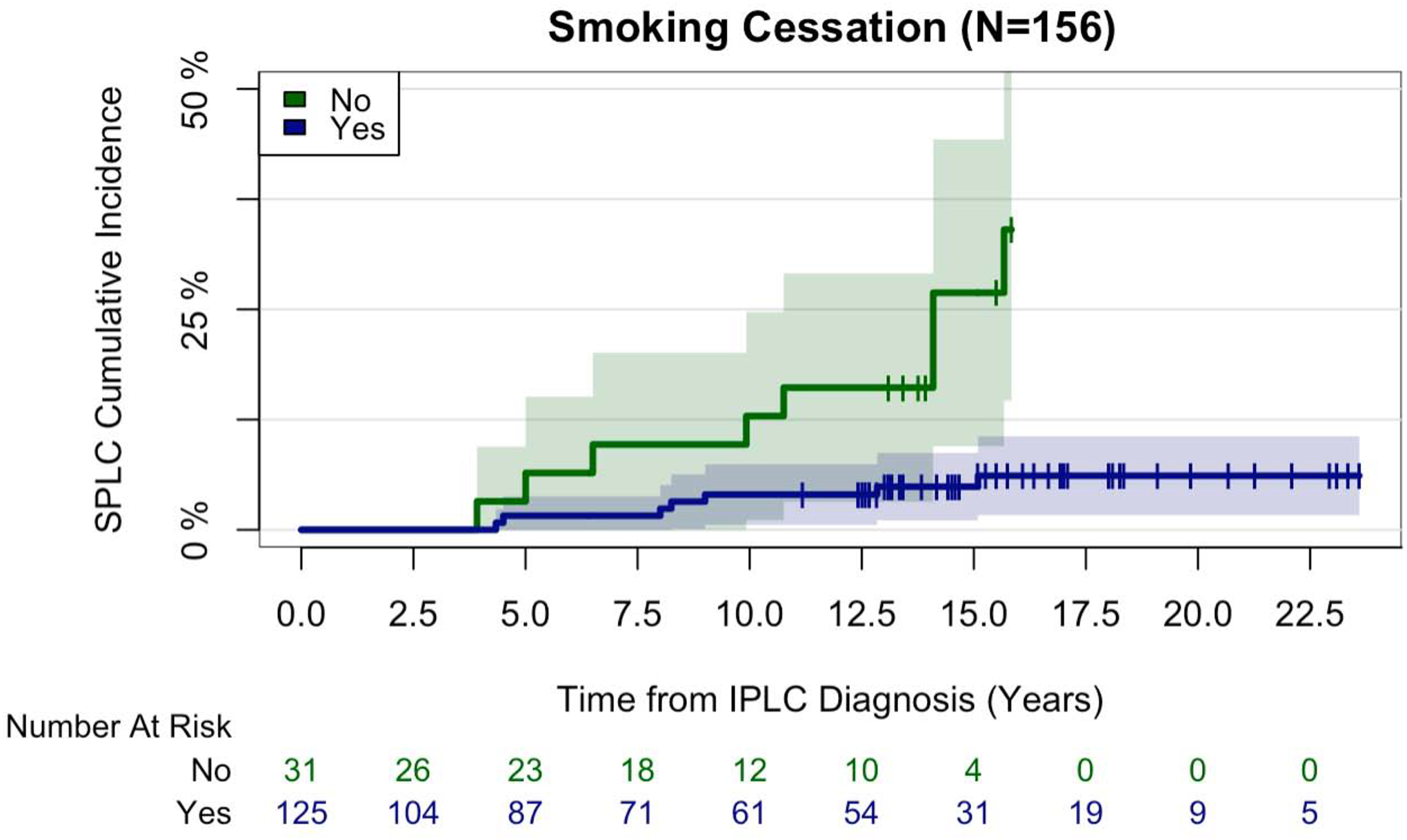
Results: Overall, 163 MEC cases (2.3%) developed SPLC. Smoking pack-years (hazard ratio [HR] = 1.18 per 10 pack-years, p < 0.001) and smoking intensity (HR = 1.30 per 10 cigarettes per day, p < 0.001) were significantly associated with increased SPLC risk. Individuals who met the 2013 U.S. Preventive Services Task Force's screening criteria at IPLC diagnosis also had an increased SPLC risk (HR = 1.92; p < 0.001). Validation studies with the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial and European Prospective Investigation into Cancer and Nutrition revealed consistent results. Meta-analysis yielded pooled HRs of 1.16 per 10 pack-years (pmeta < 0.001), 1.25 per 10 cigarettes per day (pmeta < 0.001), and 1.99 (pmeta < 0.001) for meeting the U.S. Preventive Services Task Force's criteria. In MEC, smoking cessation after IPLC diagnosis was associated with an 83% reduction in SPLC risk (HR = 0.17; p < 0.001).
Conclusions: Tobacco smoking is a risk factor for SPLC. Smoking cessation may reduce the risk of SPLC. Additional strategies for SPLC surveillance and screening are warranted.
Keywords: Screening; Second primary lung cancer; Smoking cessation; Surveillance; Tobacco smoking.
Copyright © 2021 International Association for the Study of Lung Cancer. All rights reserved.
Figures
Comment in
-
Critical Determinants of Cancer Treatment Outcomes: Smoking Must Be Addressed at the Highest Levels in Cancer Care.J Thorac Oncol. 2021 Jun;16(6):891-893. doi: 10.1016/j.jtho.2021.03.010. Epub 2021 Apr 22. J Thorac Oncol. 2021. PMID: 33895106 No abstract available.
-
Over-Time Risk of Lung Cancer Is Largely Owing to Continuing Smoking Exposition: A Good Reason to Quit.J Thorac Oncol. 2021 Aug;16(8):e57-e59. doi: 10.1016/j.jtho.2021.04.013. J Thorac Oncol. 2021. PMID: 34304855 No abstract available.
-
A Moving Target: Integration of Smoking Cessation Into Screening for Second Primary Lung Cancer.J Thorac Oncol. 2021 Aug;16(8):e59-e60. doi: 10.1016/j.jtho.2021.05.008. J Thorac Oncol. 2021. PMID: 34304856 Free PMC article. No abstract available.
References
-
- American Lung Association. State of Lung Cancer. 2019.
-
- Johnson BE. Second lung cancers in patients after treatment for an initial lung cancer. J Natl Cancer Inst 1998;90:1335–1345. - PubMed
-
- Surapaneni R, Singh P, Rajagopalan K, et al. Stage I lung cancer survivorship: risk of second malignancies and need for individualized care plan. J Thorac Oncol 2012;7:1252–1256. - PubMed
-
- Rice D, Kim HW, Sabichi A, et al. The risk of second primary tumors after resection of stage I nonsmall cell lung cancer. Ann Thorac Surg 2003;76:1001–1007; discussion 1007–1008. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
