

Approaches, enablers, barriers and outcomes of implementing facility-based stillbirth and neonatal death audit in LMICs: a systematic review
- PMID: 33722879
- PMCID: PMC7970257
- DOI: 10.1136/bmjoq-2020-001266
Approaches, enablers, barriers and outcomes of implementing facility-based stillbirth and neonatal death audit in LMICs: a systematic review
Abstract
Purpose: To identify approaches, enablers, barriers and outcomes of facility stillbirth and neonatal death audit in low-income and middle-income countries (LMICs).
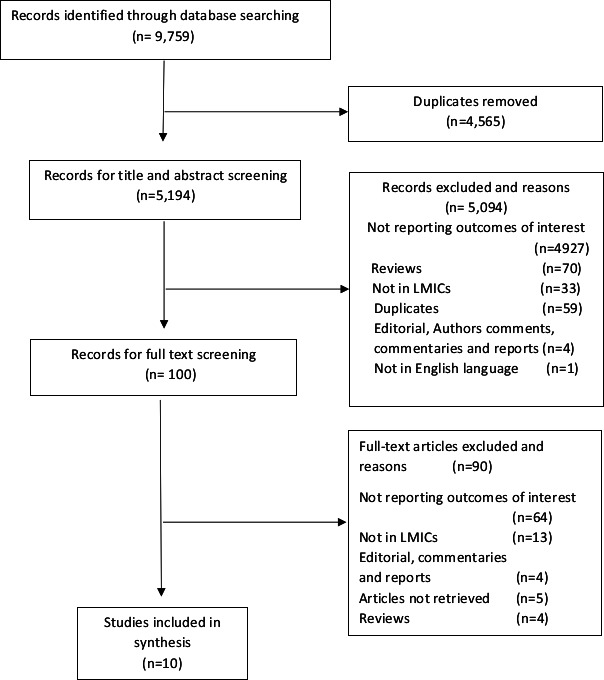
Data sources: We searched MEDLINE, CINAHL Complete, Academic Search Index, Science Citation Index, Complementary index and Global health electronic databases.
Study selection: Studies were considered eligible when reporting the approaches, enablers, barriers and outcomes of facility-based stillbirth and neonatal death audit in LMICs.
Data extraction: Two authors independently performed the data extraction using predefined templates made before data extraction.
Results of data synthesis: A total of 10 articles from 7 countries were included in the final analysis. Facility or external multidisciplinary teams performed death audits on a weekly or monthly basis. A total of 1018 stillbirths and neonatal deaths were audited. Of 18 audit enablers identified, nine were at the health provider level while 18 of 23 barriers to audit that were identified occurred at the facility level. The facility-level barriers cited by more than one study included: failure to implement change; inadequate training; limited time; increased workload; too many cases and poor documentation. Six studies reported that death audits resulted in structural improvements in physical structure, training, service organisation, supplies and equipment in the wards. Five studies reported that death audits improved the standard of care, with one study showing a significant improvement in measured standards. One study reported a significant reduction in newborn mortality rate of 29.4% (95% CI 0.6% to 2.4%; p=0.0015) and one study a reduction in perinatal mortality of 4.9% (52.8% in 2007 to 47.9% in 2008) before and after perinatal audit implementation.
Conclusion: Stillbirth and neonatal death audit improves facility structures, processes of care and health outcomes in neonatal care. There is a need to enhance enablers and address barriers identified at both health provider and facility levels to improve the audit process.
Keywords: audit and feedback; clinical audit; hospital medicine; hospital mortality; infant mortality.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Perinatal mortality audits and reporting of perinatal deaths: systematic review of outcomes and barriers.J Perinat Med. 2022 Jan 26;50(6):684-712. doi: 10.1515/jpm-2021-0363. Print 2022 Jul 26. J Perinat Med. 2022. PMID: 35086187
-
Induction of labour for improving birth outcomes for women at or beyond term.Cochrane Database Syst Rev. 2018 May 9;5(5):CD004945. doi: 10.1002/14651858.CD004945.pub4. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2020 Jul 15;7:CD004945. doi: 10.1002/14651858.CD004945.pub5. PMID: 29741208 Free PMC article. Updated.
-
Non-clinical interventions for reducing unnecessary caesarean section.Cochrane Database Syst Rev. 2018 Sep 28;9(9):CD005528. doi: 10.1002/14651858.CD005528.pub3. Cochrane Database Syst Rev. 2018. PMID: 30264405 Free PMC article.
-
Acute tocolysis for uterine tachysystole or suspected fetal distress.Cochrane Database Syst Rev. 2018 Jul 4;7(7):CD009770. doi: 10.1002/14651858.CD009770.pub2. Cochrane Database Syst Rev. 2018. PMID: 29971813 Free PMC article.
-
Maternal postures for fetal malposition in labour for improving the health of mothers and their infants.Cochrane Database Syst Rev. 2022 Aug 31;8(8):CD014615. doi: 10.1002/14651858.CD014615. Cochrane Database Syst Rev. 2022. PMID: 36043437 Free PMC article.
Cited by
-
Resource availability and barriers to delivering quality care for newborns in hospitals in the southern region of Malawi: A multisite observational study.PLOS Glob Public Health. 2022 Dec 5;2(12):e0001333. doi: 10.1371/journal.pgph.0001333. eCollection 2022. PLOS Glob Public Health. 2022. PMID: 36962885 Free PMC article.
-
Risk factors of stillbirths in four district hospitals on Pemba Island, Tanzania: a prospective cohort study.BMC Pregnancy Childbirth. 2023 Apr 26;23(1):288. doi: 10.1186/s12884-023-05613-6. BMC Pregnancy Childbirth. 2023. PMID: 37101264 Free PMC article.
-
'There is trauma all round': A qualitative study of health workers' experiences of caring for parents after stillbirth in Kenya and Uganda.Women Birth. 2023 Feb;36(1):56-62. doi: 10.1016/j.wombi.2022.02.012. Epub 2022 Mar 16. Women Birth. 2023. PMID: 35305917 Free PMC article.
-
Factors influencing maternal death surveillance and review implementation in Dodoma City, Tanzania. A qualitative case study.Learn Health Syst. 2023 Sep 4;8(2):e10390. doi: 10.1002/lrh2.10390. eCollection 2024 Apr. Learn Health Syst. 2023. PMID: 38633026 Free PMC article.
-
Factors impacting-stillbirth and neonatal death audit in Malawi: a qualitative study.BMC Health Serv Res. 2022 Sep 22;22(1):1191. doi: 10.1186/s12913-022-08578-y. BMC Health Serv Res. 2022. PMID: 36138396 Free PMC article.
References
-
- UN IGME, Levels & Trends in Child mortality Report 2020, UNICEF, et al., Editors. 2020: New York, US.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials