

Thin-Layer-Agar-Based Direct Phenotypic Drug Susceptibility Testing on Sputum in Eswatini Rapidly Detects Mycobacterium tuberculosis Growth and Rifampicin Resistance Otherwise Missed by WHO-Endorsed Diagnostic Tests
- PMID: 33722892
- PMCID: PMC8315964
- DOI: 10.1128/AAC.02263-20
Thin-Layer-Agar-Based Direct Phenotypic Drug Susceptibility Testing on Sputum in Eswatini Rapidly Detects Mycobacterium tuberculosis Growth and Rifampicin Resistance Otherwise Missed by WHO-Endorsed Diagnostic Tests
Abstract
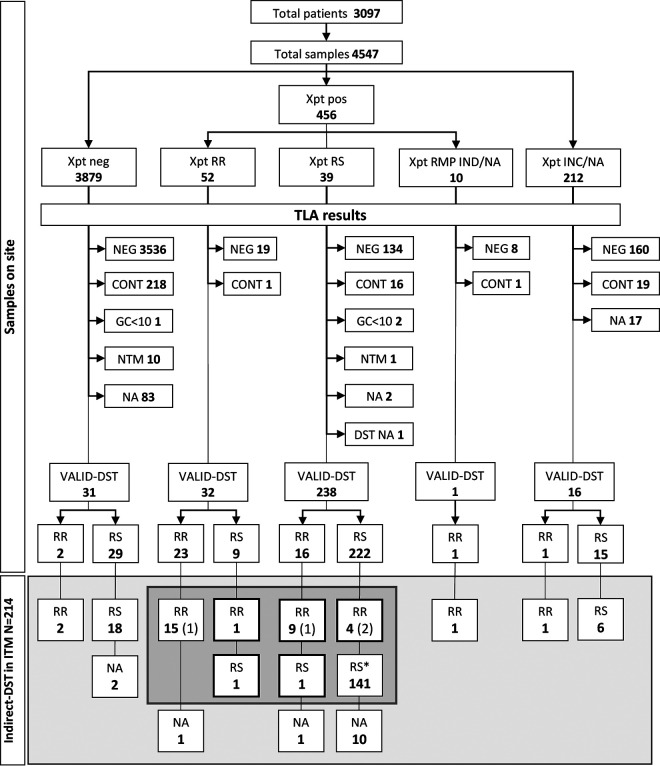
Xpert MTB/RIF rapidly detects resistance to rifampicin (RR); however, this test misses I491F-RR conferring rpoB mutation, common in southern Africa. In addition, Xpert MTB/RIF does not distinguish between viable and dead Mycobacterium tuberculosis (MTB). We aimed to investigate the ability of thin-layer agar (TLA) direct drug-susceptibility testing (DST) to detect MTB and its drug-resistance profiles in field conditions in Eswatini. Consecutive samples were tested in parallel with Xpert MTB/RIF and TLA for rifampicin (1.0 μg/ml) and ofloxacin (2.0 μg/ml). TLA results were compared at the Reference Laboratory in Antwerp with indirect-DST on Löwenstein-Jensen or 7H11 solid media and additional phenotypic and genotypic testing to resolve discordance. TLA showed a positivity rate for MTB detection of 7.1% versus 10.0% for Xpert MTB/RIF. Of a total of 4,547 samples included in the study, 200 isolates were available for comparison to the composite reference. Within a median of 18.4 days, TLA detected RR with 93.0% sensitivity (95% confidence interval [CI], 77.4 to 98.0) and 99.4% specificity (95% CI, 96.7 to 99.9) versus 62.5% (95% CI, 42.7 to 78.8) and 99.3% (95% CI, 96.2 to 99.9) for Xpert MTB/RIF. Eight isolates, 28.6% of all RR-confirmed isolates, carried the I491F mutation, all detected by TLA. TLA also correctly identified 183 of the 184 ofloxacin-susceptible isolates (99.5% specificity; 95% CI, 97.0 to 99.9). In field conditions, TLA rapidly detects RR, and in this specific setting, it contributed to detection of additional RR patients over Xpert MTB/RIF, mainly but not exclusively due to I491F. TLA also accurately excluded fluoroquinolone resistance.
Keywords: MDR; TLA; XDR; Xpert MTB/RIF; resistance detection; rpoB I491F mutant; tuberculosis.
Copyright © 2021 Ardizzoni et al.
Figures
Similar articles
-
Rifampicin resistance mutations in the 81 bp RRDR of rpoB gene in Mycobacterium tuberculosis clinical isolates using Xpert® MTB/RIF in Kampala, Uganda: a retrospective study.BMC Infect Dis. 2014 Sep 4;14:481. doi: 10.1186/1471-2334-14-481. BMC Infect Dis. 2014. PMID: 25190040 Free PMC article.
-
[Evaluation of the performance of InnowaveDX MTB/RIF for the detection of Mycobacterium tuberculosis complex and rifampicin resistance].Zhonghua Jie He He Hu Xi Za Zhi. 2023 Jul 12;46(7):658-663. doi: 10.3760/cma.j.cn112147-20221104-00877. Zhonghua Jie He He Hu Xi Za Zhi. 2023. PMID: 37402655 Chinese.
-
The New Xpert MTB/RIF Ultra: Improving Detection of Mycobacterium tuberculosis and Resistance to Rifampin in an Assay Suitable for Point-of-Care Testing.mBio. 2017 Aug 29;8(4):e00812-17. doi: 10.1128/mBio.00812-17. mBio. 2017. PMID: 28851844 Free PMC article.
-
Xpert Ultra versus Xpert MTB/RIF for pulmonary tuberculosis and rifampicin resistance in adults with presumptive pulmonary tuberculosis.Cochrane Database Syst Rev. 2021 Feb 22;2(2):CD009593. doi: 10.1002/14651858.CD009593.pub5. Cochrane Database Syst Rev. 2021. PMID: 33616229 Free PMC article.
-
Truenat MTB assays for pulmonary tuberculosis and rifampicin resistance in adults and adolescents.Cochrane Database Syst Rev. 2025 Mar 24;3(3):CD015543. doi: 10.1002/14651858.CD015543.pub2. Cochrane Database Syst Rev. 2025. PMID: 40122135 Free PMC article. Review.
Cited by
-
Evolution of Mycobacterium tuberculosis drug resistance in the genomic era.Front Cell Infect Microbiol. 2022 Oct 7;12:954074. doi: 10.3389/fcimb.2022.954074. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36275027 Free PMC article. Review.
-
Exploring programmatic indicators of tuberculosis control that incorporate routine Mycobacterium tuberculosis sequencing in low incidence settings: a comprehensive (2017-2021) patient cohort analysis.Lancet Reg Health West Pac. 2023 Sep 27;41:100910. doi: 10.1016/j.lanwpc.2023.100910. eCollection 2023 Dec. Lancet Reg Health West Pac. 2023. PMID: 37808343 Free PMC article.
-
Clinical standards for drug-susceptible pulmonary TB.Int J Tuberc Lung Dis. 2022 Jul 1;26(7):592-604. doi: 10.5588/ijtld.22.0228. Int J Tuberc Lung Dis. 2022. PMID: 35768923 Free PMC article.
-
Rapid Diagnostic Sequencing of Stool DNA Using Targeted Nanopore Sequencing in Patients With a Pulmonary Tuberculosis Diagnosis.Open Forum Infect Dis. 2025 Mar 6;12(4):ofaf121. doi: 10.1093/ofid/ofaf121. eCollection 2025 Apr. Open Forum Infect Dis. 2025. PMID: 40212033 Free PMC article.
-
Drug resistance of Mycobacterium tuberculosis to linezolid and delamanid: a case report from Bukavu, Democratic Republic of Congo.BMC Infect Dis. 2025 Jul 12;25(1):913. doi: 10.1186/s12879-025-11348-w. BMC Infect Dis. 2025. PMID: 40652177 Free PMC article.
References
-
- World Health Organization. 2020. Global tuberculosis report. World Health Organization, Geneva, Switzerland.
-
- Global Laboratory Initiative. 2018. Line probe assays for drug-resistant tuberculosis detection. Interpretation and reporting guide for laboratory staff and clinicians. Global TB Programme, World Health Organization, Geneva, Switzerland. http://www.stoptb.org/wg/gli/assets/documents/LPA_test_web_ready.pdf.
-
- Cox H, Dickson-Hall L, Ndjeka N, van’t Hoog A, Grant A, Cobelens F, Stevens W, Nicol M. 2017. Delays and loss to follow-up before treatment of drug-resistant tuberculosis following implementation of Xpert MTB/RIF in South Africa: a retrospective cohort study. PLoS Med 14:e1002238-19. 10.1371/journal.pmed.1002238. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
