

Phase I/II Trial of Exemestane, Ribociclib, and Everolimus in Women with HR+/HER2- Advanced Breast Cancer after Progression on CDK4/6 Inhibitors (TRINITI-1)
- PMID: 33722897
- PMCID: PMC8487593
- DOI: 10.1158/1078-0432.CCR-20-2114
Phase I/II Trial of Exemestane, Ribociclib, and Everolimus in Women with HR+/HER2- Advanced Breast Cancer after Progression on CDK4/6 Inhibitors (TRINITI-1)
Abstract
Purpose: Standard-of-care treatment for metastatic hormone receptor-positive (HR+), HER2-negative (HER2-) breast cancer includes endocrine therapy (ET) combined with a cyclin-dependent kinase 4/6 inhibitor (CDK4/6i). Optimal treatment after progression on CDK4/6i is unknown. The TRINITI-1 trial investigated ribociclib, a CDK4/6i that has recently demonstrated significant overall survival benefit in two phase III trials, in combination with everolimus and exemestane in patients with HR+, HER2- advanced breast cancer (ABC) after progression on a CDK4/6i.
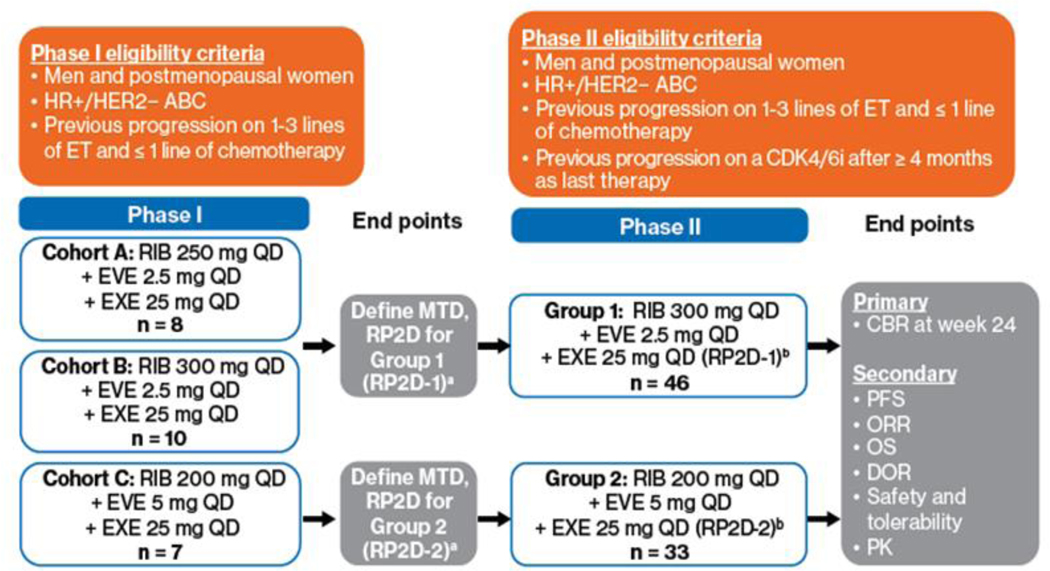
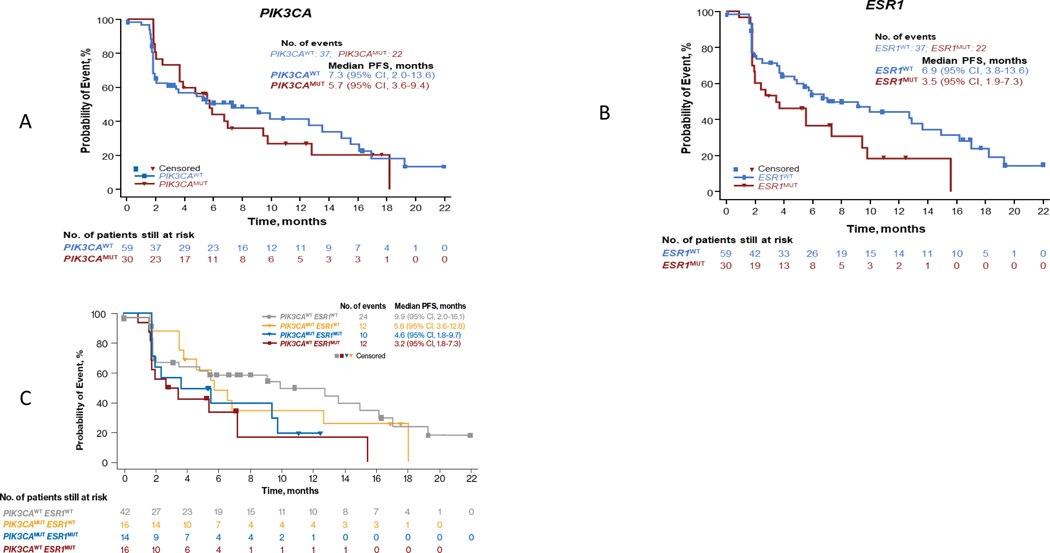
Patients and methods: This multicenter, open-label, single-arm, phase I/II study included patients with locally advanced/metastatic HR+/HER2- breast cancer. The primary endpoint was clinical benefit rate (CBR) at week 24 among patients with ET-refractory disease with progression on a CDK4/6i. Other endpoints included safety and biomarker analysis.
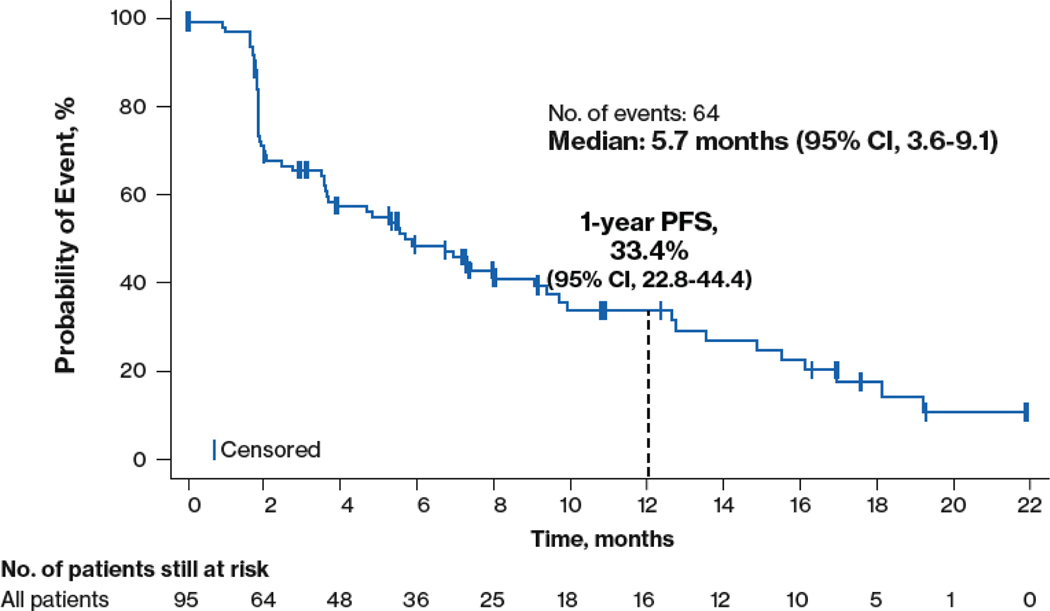
Results: Of 104 patients enrolled (phases I and II), 96 had prior CDK4/6i. Recommended phase II doses (all once daily days 1-28 of 28-day cycle) were ribociclib 300 mg, everolimus 2.5 mg, and exemestane 25 mg (group 1) and ribociclib 200 mg, everolimus 5 mg, and exemestane 25 mg (group 2). CBR among 95 efficacy-evaluable patients (phases I and II) at week 24 was 41.1% (95% confidence interval, 31.1-51.6), which met the primary endpoint (predetermined threshold: 10%). Common adverse events included neutropenia (69.2%) and stomatitis (40.4%). No new safety signals were observed; no grade 3/4 QTc prolongation was reported.
Conclusions: Preliminary TRINITI-1 safety and efficacy results support further investigation of CDK4/6 blockade and targeting of the PI3K/AKT/mTOR signaling pathway in patients with ET-refractory HR+/HER2- ABC after progression on a CDK4/6i.
©2021 American Association for Cancer Research.
Figures
References
-
- Cortes J, Im SA, Holgado E, Perez-Garcia JM, Schmid P, Chavez-MacGregor M. The next era of treatment for hormone receptor-positive, HER2-negative advanced breast cancer: triplet combination-based endocrine therapies. Cancer Treat Rev. 2017;61:53–60. - PubMed
-
- Mayer IA, Arteaga CL. The PI3K/AKT pathway as a target for cancer treatment. Annu Rev Med. 2016;67:11–28. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
