

SARS-CoV-2 infection of human iPSC-derived cardiac cells reflects cytopathic features in hearts of patients with COVID-19
- PMID: 33723017
- PMCID: PMC8128284
- DOI: 10.1126/scitranslmed.abf7872
SARS-CoV-2 infection of human iPSC-derived cardiac cells reflects cytopathic features in hearts of patients with COVID-19
Abstract
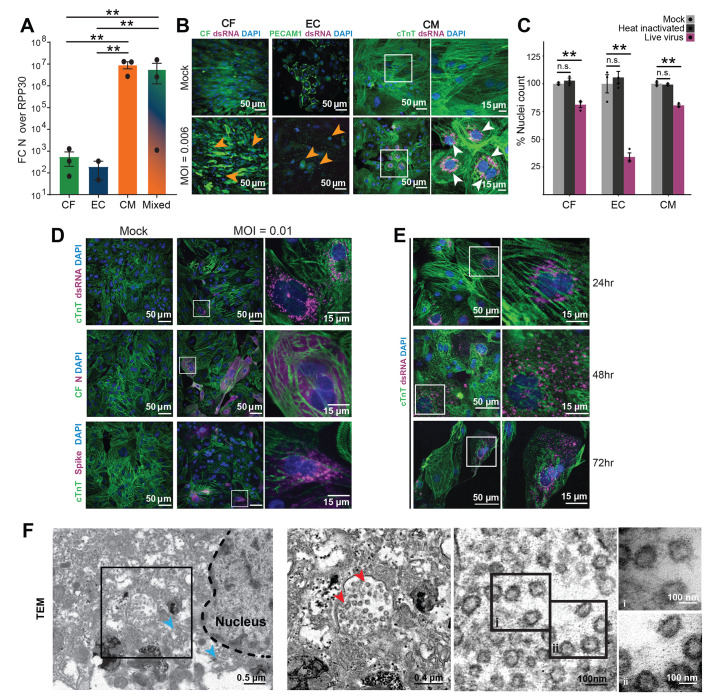
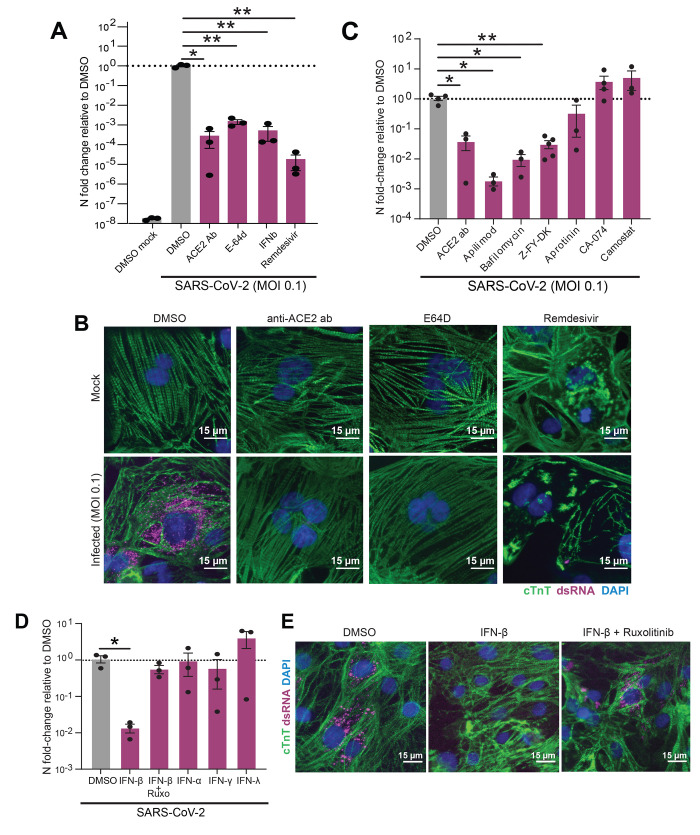
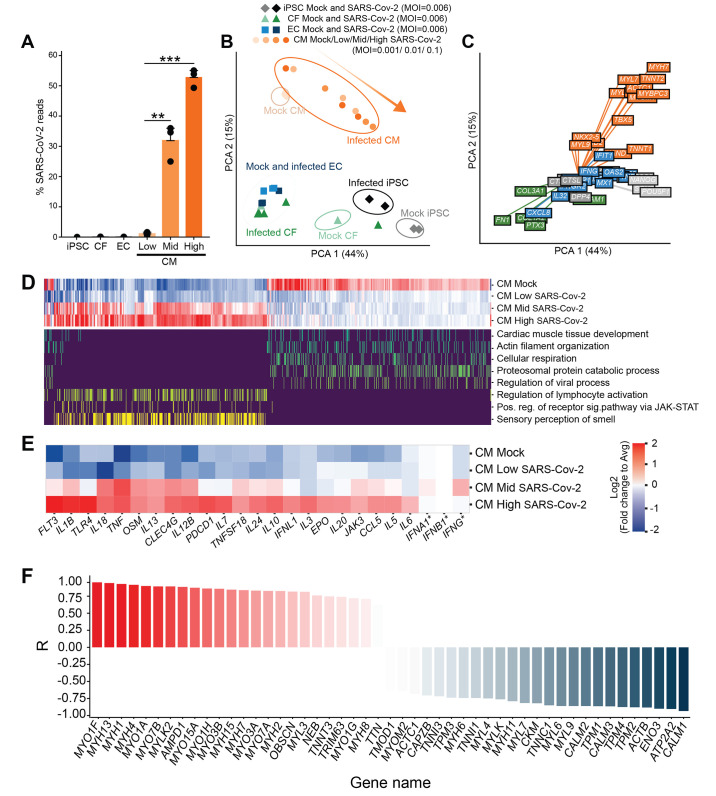
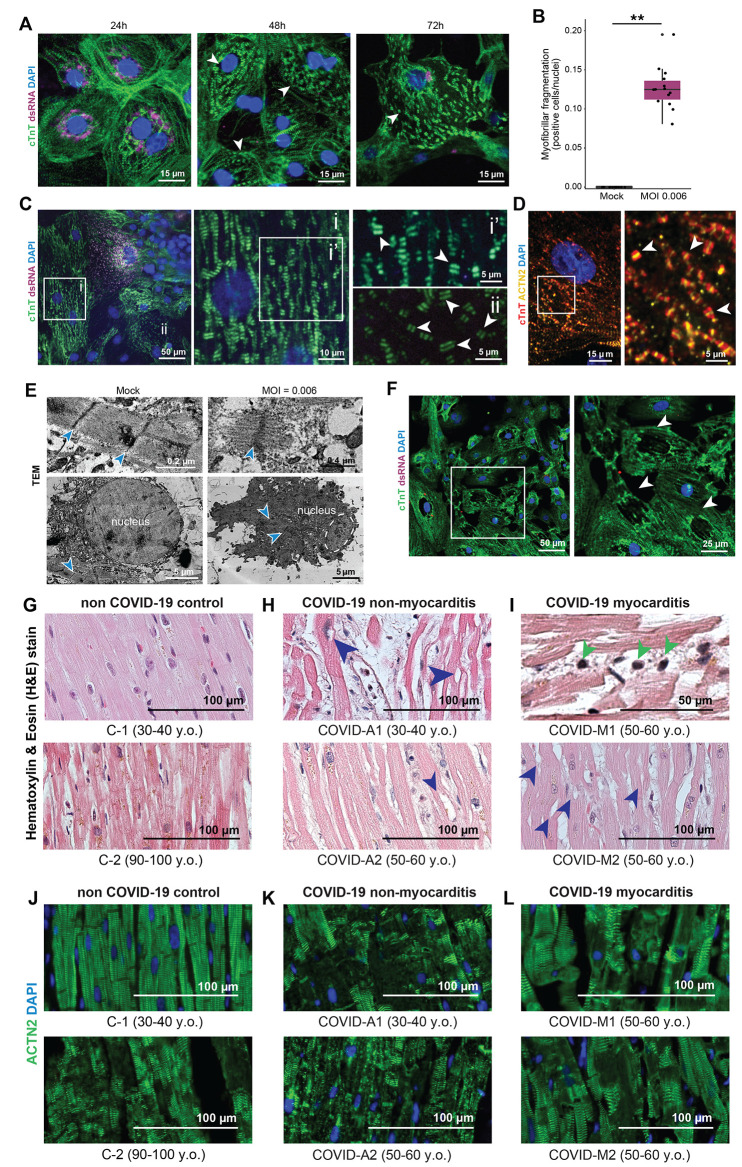
Although coronavirus disease 2019 (COVID-19) causes cardiac dysfunction in up to 25% of patients, its pathogenesis remains unclear. Exposure of human induced pluripotent stem cell (iPSC)-derived heart cells to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) revealed productive infection and robust transcriptomic and morphological signatures of damage, particularly in cardiomyocytes. Transcriptomic disruption of structural genes corroborates adverse morphologic features, which included a distinct pattern of myofibrillar fragmentation and nuclear disruption. Human autopsy specimens from patients with COVID-19 reflected similar alterations, particularly sarcomeric fragmentation. These notable cytopathic features in cardiomyocytes provide insights into SARS-CoV-2-induced cardiac damage, offer a platform for discovery of potential therapeutics, and raise concerns about the long-term consequences of COVID-19 in asymptomatic and severe cases.
Copyright © 2021 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works. Distributed under a Creative Commons Attribution License 4.0 (CC BY).
Figures
Update of
-
SARS-CoV-2 infection of human iPSC-derived cardiac cells predicts novel cytopathic features in hearts of COVID-19 patients.bioRxiv [Preprint]. 2020 Sep 12:2020.08.25.265561. doi: 10.1101/2020.08.25.265561. bioRxiv. 2020. Update in: Sci Transl Med. 2021 Apr 21;13(590):eabf7872. doi: 10.1126/scitranslmed.abf7872. PMID: 32935097 Free PMC article. Updated. Preprint.
References
-
- Wang D., Hu B., Hu C., Zhu F., Liu X., Zhang J., Wang B., Xiang H., Cheng Z., Xiong Y., Zhao Y., Li Y., Wang X., Peng Z., Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 323, 1061–1069 (2020). 10.1001/jama.2020.1585 - DOI - PMC - PubMed
-
- Chen N., Zhou M., Dong X., Qu J., Gong F., Han Y., Qiu Y., Wang J., Liu Y., Wei Y., Xia J., Yu T., Zhang X., Zhang L., Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 395, 507–513 (2020). 10.1016/S0140-6736(20)30211-7 - DOI - PMC - PubMed
-
- Fried J. A., Ramasubbu K., Bhatt R., Topkara V. K., Clerkin K. J., Horn E., Rabbani L., Brodie D., Jain S. S., Kirtane A. J., Masoumi A., Takeda K., Kumaraiah D., Burkhoff D., Leon M., Schwartz A., Uriel N., Sayer G., The variety of cardiovascular presentations of COVID-19. Circulation 141, 1930–1936 (2020). 10.1161/CIRCULATIONAHA.120.047164 - DOI - PMC - PubMed
-
- Richardson S., Hirsch J. S., Narasimhan M., Crawford J. M., McGinn T., Davidson K. W., Barnaby D. P., Becker L. B., Chelico J. D., Cohen S. L., Cookingham J., Coppa K., Diefenbach M. A., Dominello A. J., Duer-Hefele J., Falzon L., Gitlin J., Hajizadeh N., Harvin T. G., Hirschwerk D. A., Kim E. J., Kozel Z. M., Marrast L. M., Mogavero J. N., Osorio G. A., Qiu M., Zanos T. P.; the Northwell COVID-19 Research Consortium , Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 323, 2052–2059 (2020). 10.1001/jama.2020.6775 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- P01 HL089707/HL/NHLBI NIH HHS/United States
- R38 HL143581/HL/NHLBI NIH HHS/United States
- P01 HL146366/HL/NHLBI NIH HHS/United States
- ERC_/European Research Council/International
- T32 GM007618/GM/NIGMS NIH HHS/United States
- U01 ES032673/ES/NIEHS NIH HHS/United States
- 5DP1 DA038043/NH/NIH HHS/United States
- R01 HL130533/HL/NHLBI NIH HHS/United States
- R01 HL135358/HL/NHLBI NIH HHS/United States
- DP1 DA038043/DA/NIDA NIH HHS/United States
- AHA/American Heart Association-American Stroke Association/United States
- R01 AG065428/AG/NIA NIH HHS/United States
- 1R01 AG065428/NH/NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
