

Type 2 diabetes is more predictable in women than men by multiple anthropometric and biochemical measures
- PMID: 33723361
- PMCID: PMC7960723
- DOI: 10.1038/s41598-021-85581-z
Type 2 diabetes is more predictable in women than men by multiple anthropometric and biochemical measures
Abstract
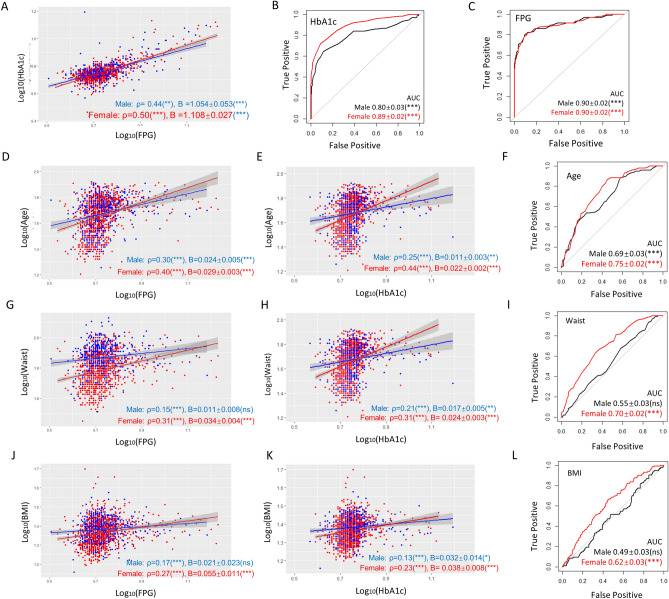
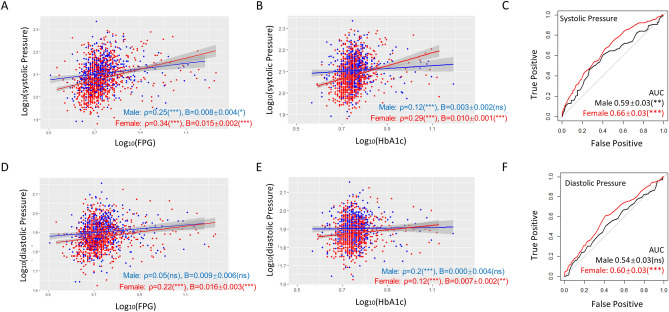
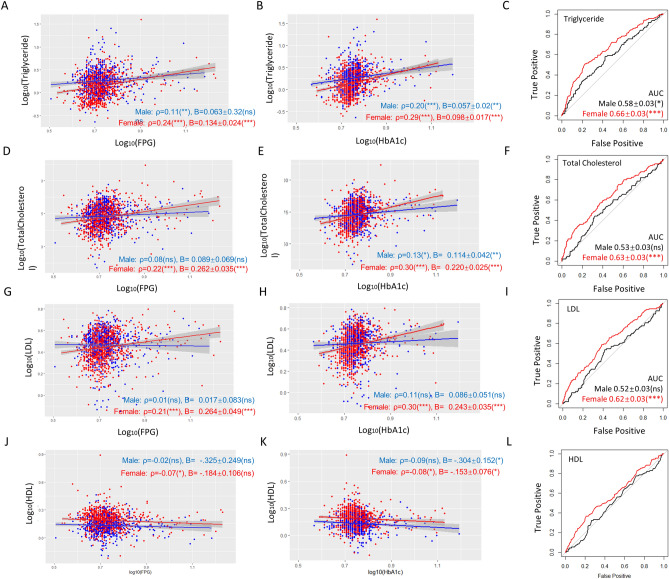
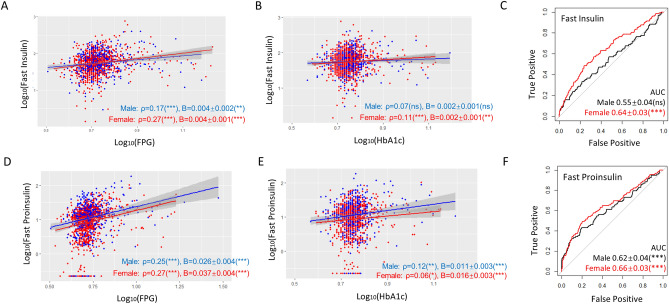
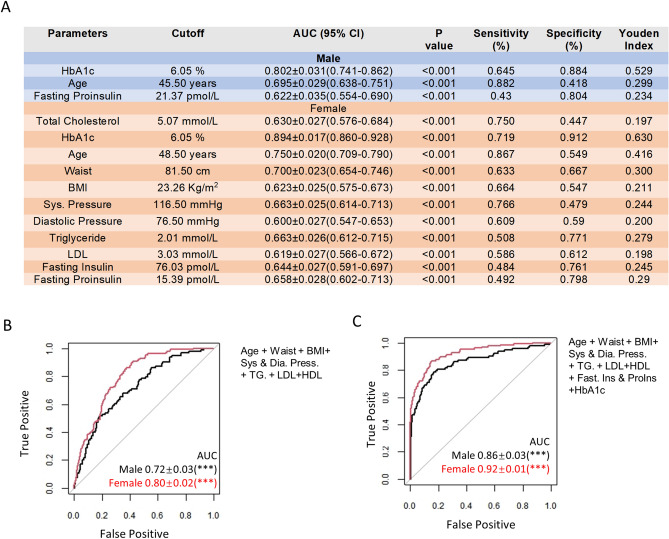
Men and women are sexually dimorphic but whether common anthropometric and biochemical parameters predict type 2 diabetes (T2D) in different ways has not been well studied. Here we recruit 1579 participants in Hainan Province, China, and group them by sex. We compared the prediction power of common parameters of T2D in two sexes by association, regression, and Receiver Operating Characteristic (ROC) analysis. HbA1c is associated with FPG stronger in women than in men and the regression coefficient is higher, consistent with higher prediction power for T2D. Age, waist circumference, BMI, systolic and diastolic blood pressure, triglyceride levels, total cholesterol, LDL, HDL, fasting insulin, and proinsulin levels all predict T2D better in women. Except for diastolic blood pressure, all parameters associate or tend to associate with FPG stronger in women than in men. Except for diastolic blood pressure and fasting proinsulin, all parameters associate or tend to associate with HbA1c stronger in women than in men. Except for fasting proinsulin and HDL, the regression coefficients of all parameters with FPG and HbA1c were higher in women than in men. Together, by the above anthropometric and biochemical measures, T2D is more readily predicted in women than men, suggesting the importance of sex-based subgroup analysis in T2D research.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- American Diabetes, A. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care42, S13-S28. 10.2337/dc19-S002 (2019). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
