

Cost-effectiveness of an enhanced Paramedic Acute Stroke Treatment Assessment (PASTA) during emergency stroke care: Economic results from a pragmatic cluster randomized trial
- PMID: 33724103
- PMCID: PMC8864331
- DOI: 10.1177/17474930211006302
Cost-effectiveness of an enhanced Paramedic Acute Stroke Treatment Assessment (PASTA) during emergency stroke care: Economic results from a pragmatic cluster randomized trial
Abstract
Background: The Paramedic Acute Stroke Treatment Assessment (PASTA) trial evaluated an enhanced emergency care pathway which aimed to facilitate thrombolysis in hospital. A pre-planned health economic evaluation was included. The main results showed no statistical evidence of a difference in either thrombolysis volume (primary outcome) or 90-day dependency. However, counter-intuitive findings were observed with the intervention group showing fewer thrombolysis treatments but less dependency.
Aims: Cost-effectiveness of the PASTA intervention was examined relative to standard care.
Methods: A within trial cost-utility analysis estimated mean costs and quality-adjusted life years over 90 days' time horizon. Costs were derived from resource utilization data for individual trial participants. Quality-adjusted life years were calculated by mapping modified Rankin scale scores to EQ-5D-3L utility tariffs. A post-hoc subgroup analysis examined cost-effectiveness when trial hospitals were divided into compliant and non-compliant with recommendations for a stroke specialist thrombolysis rota.
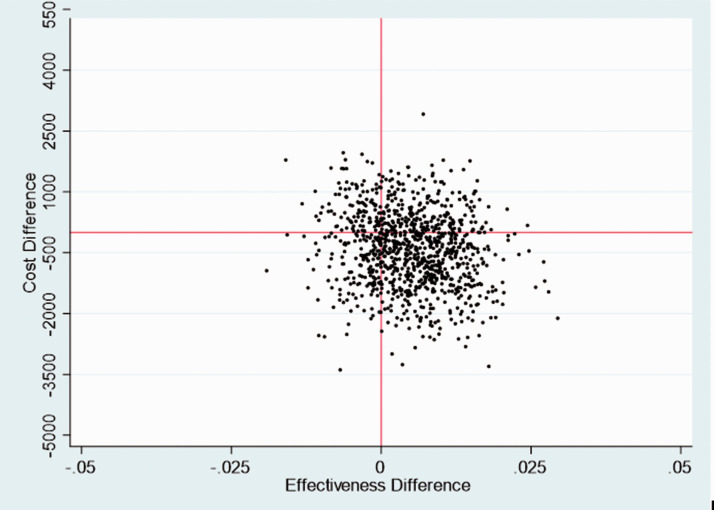
Results: The trial enrolled 1214 patients: 500 PASTA and 714 standard care. There was no evidence of a quality-adjusted life year difference between groups [0·007 (95% CI: -0·003 to 0·018)] but costs were lower in the PASTA group [-£1473 (95% CI: -£2736 to -£219)]. There was over 97.5% chance that the PASTA pathway would be considered cost-effective. There was no evidence of a difference in costs at seven thrombolysis rota compliant hospitals but costs at eight non-complaint hospitals costs were lower in PASTA with more dominant cost-effectiveness.
Conclusions: Analyses indicate that the PASTA pathway may be considered cost-effective, particularly if deployed in areas where stroke specialist availability is limited.Trial Registration: ISRCTN12418919 www.isrctn.com/ISRCTN12418919.
Keywords: Stroke; ambulance; cluster randomized controlled trial; cost-effectiveness; paramedic; thrombolysis.
Conflict of interest statement
Figures



Similar articles
-
Effect of an Enhanced Paramedic Acute Stroke Treatment Assessment on Thrombolysis Delivery During Emergency Stroke Care: A Cluster Randomized Clinical Trial.JAMA Neurol. 2020 Jul 1;77(7):840-848. doi: 10.1001/jamaneurol.2020.0611. JAMA Neurol. 2020. PMID: 32282015 Free PMC article. Clinical Trial.
-
Paramedic Acute Stroke Treatment Assessment (PASTA): study protocol for a randomised controlled trial.Trials. 2019 Feb 12;20(1):121. doi: 10.1186/s13063-018-3144-z. Trials. 2019. PMID: 30755249 Free PMC article.
-
Prehospital Telestroke vs Paramedic Scores to Accurately Identify Stroke Reperfusion Candidates: A Cluster Randomized Controlled Trial.Neurology. 2022 Nov 8;99(19):e2125-e2136. doi: 10.1212/WNL.0000000000201104. Epub 2022 Aug 31. Neurology. 2022. PMID: 36240100 Clinical Trial.
-
Paramedic experiences of using an enhanced stroke assessment during a cluster randomised trial: a qualitative thematic analysis.Emerg Med J. 2020 Aug;37(8):480-485. doi: 10.1136/emermed-2019-209392. Epub 2020 Jun 16. Emerg Med J. 2020. PMID: 32546477 Free PMC article. Clinical Trial.
-
The integrated care pathway for managing post stroke patients (iCaPPS©) in public primary care Healthcentres in Malaysia: impact on quality adjusted life years (QALYs) and cost effectiveness analysis.BMC Geriatr. 2020 Feb 18;20(1):70. doi: 10.1186/s12877-020-1453-z. BMC Geriatr. 2020. PMID: 32070291 Free PMC article.
Cited by
-
The World Stroke Academy: A World Stroke Organization global pathway to improve knowledge in stroke care.Int J Stroke. 2022 Oct;17(8):829-834. doi: 10.1177/17474930221085895. Epub 2022 Mar 10. Int J Stroke. 2022. PMID: 35195047 Free PMC article. Review.
References
-
- Sentinel Stroke National Audit Programme. School of Population Health and Environmental Studies King’s College London, https://www.strokeaudit.org.
-
- Wojner-Alexandrov AW, Alexandrov AV, Rodriguez D, Persse D, Grotta JC. Houston paramedic and emergency stroke treatment and outcomes study (HoPSTO). Stroke 2005; 36: 1512–1518. - PubMed
-
- Berglund A, Svensson L, Sjostrand C, et al. Higher prehospital priority level of stroke improves thrombolysis frequency and time to stroke unit: The Hyper Acute STroke Alarm (HASTA) Study. Stroke 2012; 43: 2666–2670. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
