

Serum Glial Fibrillary Acidic Protein: A Neuromyelitis Optica Spectrum Disorder Biomarker
- PMID: 33724534
- PMCID: PMC8252046
- DOI: 10.1002/ana.26067
Serum Glial Fibrillary Acidic Protein: A Neuromyelitis Optica Spectrum Disorder Biomarker
Abstract
Objective: Blood tests to monitor disease activity, attack severity, or treatment impact in neuromyelitis optica spectrum disorder (NMOSD) have not been developed. This study investigated the relationship between serum glial fibrillary acidic protein (sGFAP) concentration and NMOSD activity and assessed the impact of inebilizumab treatment.
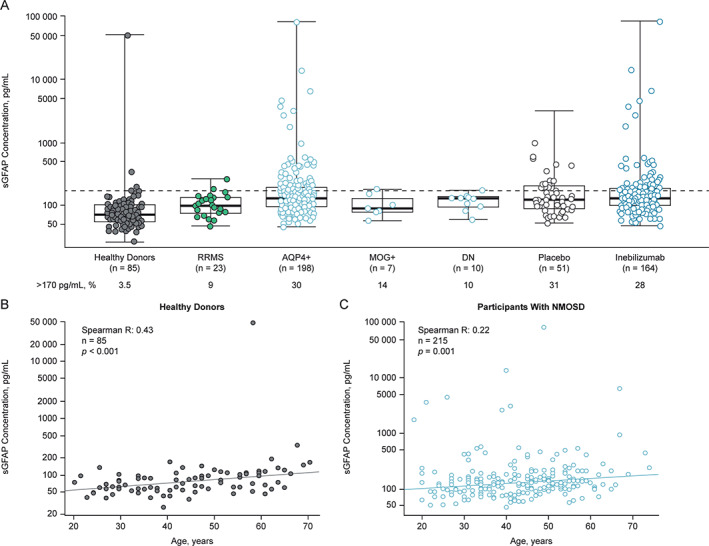
Methods: N-MOmentum was a prospective, multicenter, double-blind, placebo-controlled, randomized clinical trial in adults with NMOSD. sGFAP levels were measured by single-molecule arrays (SIMOA) in 1,260 serial and attack-related samples from 215 N-MOmentum participants (92% aquaporin 4-immunoglobulin G-seropositive) and in control samples (from healthy donors and patients with relapsing-remitting multiple sclerosis).
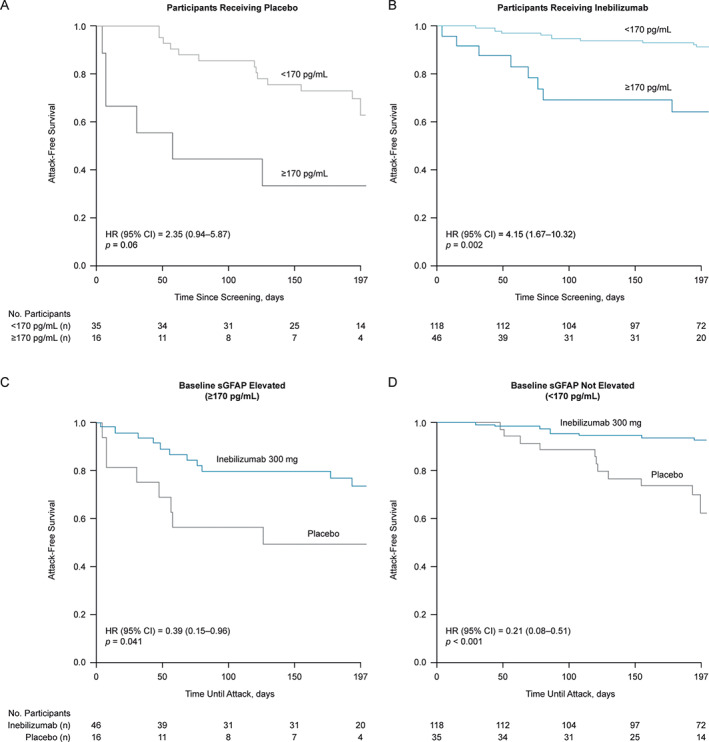
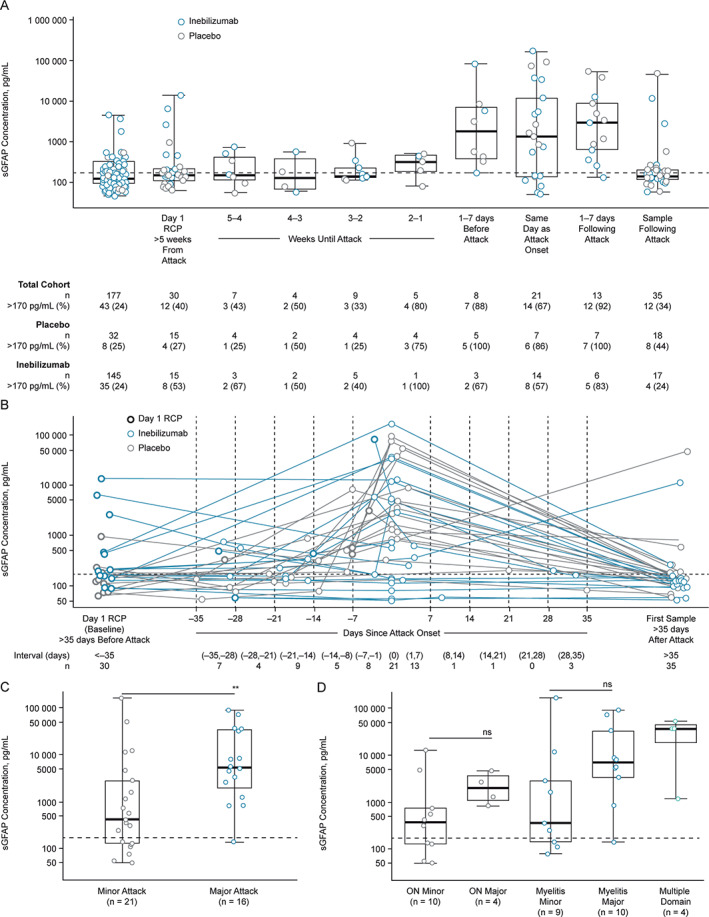
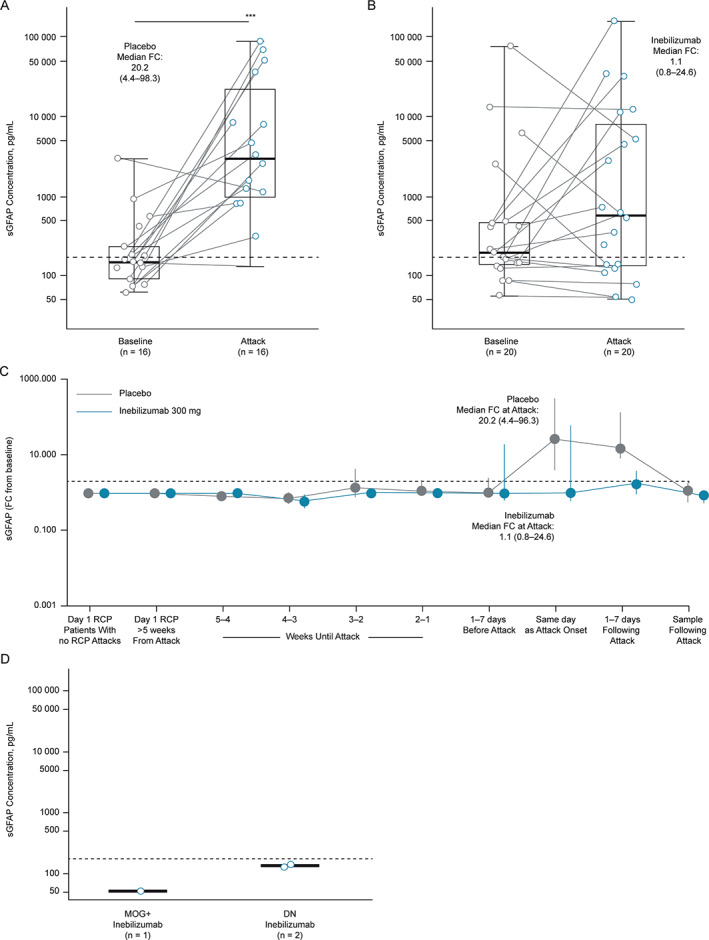
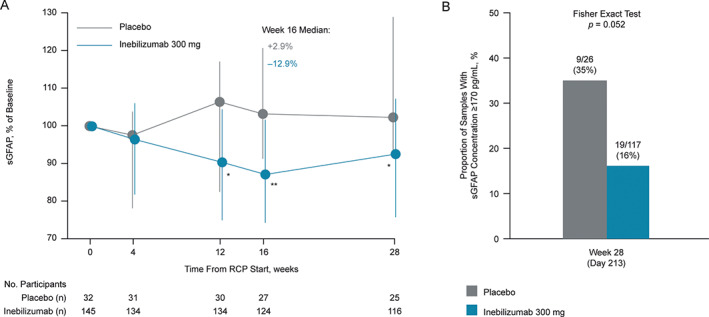
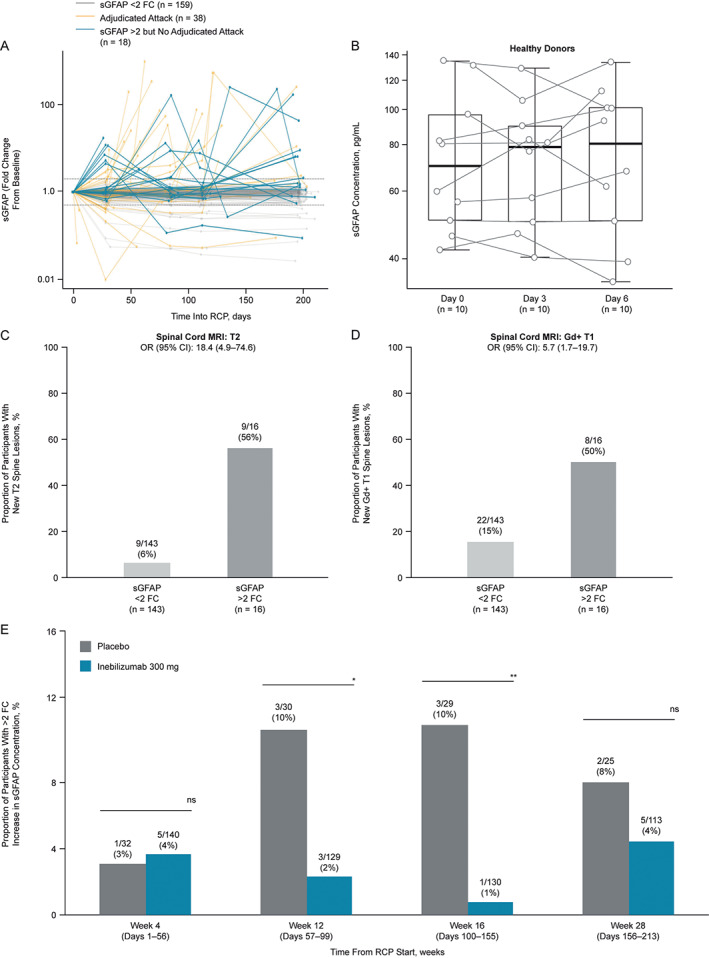
Results: At baseline, 62 participants (29%) exhibited high sGFAP concentrations (≥170 pg/ml; ≥2 standard deviations above healthy donor mean concentration) and were more likely to experience an adjudicated attack than participants with lower baseline concentrations (hazard ratio [95% confidence interval], 3.09 [1.6-6.1], p = 0.001). Median (interquartile range [IQR]) concentrations increased within 1 week of an attack (baseline: 168.4, IQR = 128.9-449.7 pg/ml; attack: 2,160.1, IQR = 302.7-9,455.0 pg/ml, p = 0.0015) and correlated with attack severity (median fold change from baseline [FC], minor attacks: 1.06, IQR = 0.9-7.4; major attacks: 34.32, IQR = 8.7-107.5, p = 0.023). This attack-related increase in sGFAP occurred primarily in placebo-treated participants (FC: 20.2, IQR = 4.4-98.3, p = 0.001) and was not observed in inebilizumab-treated participants (FC: 1.1, IQR = 0.8-24.6, p > 0.05). Five participants (28%) with elevated baseline sGFAP reported neurological symptoms leading to nonadjudicated attack assessments.
Interpretation: Serum GFAP may serve as a biomarker of NMOSD activity, attack risk, and treatment effects. ANN NEUROL 2021;89:895-910.
Trial registration: ClinicalTrials.gov NCT02200770.
© 2021 The Authors. Annals of Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
Viela Bio and MedImmune funded the N‐MOmentum study. Viela Bio is the owner of inebilizumab. Mitsubishi Tanabe Pharma Corporation and Hansoh Pharmaceutical Group Co. Ltd. have partnerships with Viela Bio to develop and commercialize inebilizumab for NMOSD (and other potential indications) in Asia. O.A. serves on a steering committee for Viela Bio and has received funding for travel and fees from Viela Bio. M.A.S., W.R., D.S., and E.K. are employees of Viela Bio. J.L.B. reports payment for study design/consultation from Viela Bio and personal fees from Mitsubishi Tanabe Pharma Corporation. B.A.C.C. has nothing to report.
Figures
References
-
- Cree BA, Lamb S, Morgan K, et al. An open label study of the effects of rituximab in neuromyelitis optica. Neurology 2005;64:1270–1272. - PubMed
-
- Damato V, Evoli A, Iorio R. Efficacy and safety of rituximab therapy in neuromyelitis optica spectrum disorders: a systematic review and meta‐analysis. JAMA Neurol 2016;73:1342–1348. - PubMed
-
- Tahara M, Oeda T, Okada K, et al. Safety and efficacy of rituximab in neuromyelitis optica spectrum disorders (RIN‐1 study): a multicentre, randomised, double‐blind, placebo‐controlled trial. Lancet Neurol 2020;19:298–306. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
