

Risk of requiring a walking aid after 6.5 years of ocrelizumab treatment in patients with relapsing multiple sclerosis: Data from the OPERA I and OPERA II trials
- PMID: 33724637
- PMCID: PMC9290576
- DOI: 10.1111/ene.14823
Risk of requiring a walking aid after 6.5 years of ocrelizumab treatment in patients with relapsing multiple sclerosis: Data from the OPERA I and OPERA II trials
Abstract
Background and purpose: Requiring a walking aid is a fundamental milestone in multiple sclerosis (MS), represented by an Expanded Disability Status Scale (EDSS) score ≥6.0. In the present study, we assess the effect of ocrelizumab (OCR) on time to EDSS score ≥6.0 in relapsing MS.
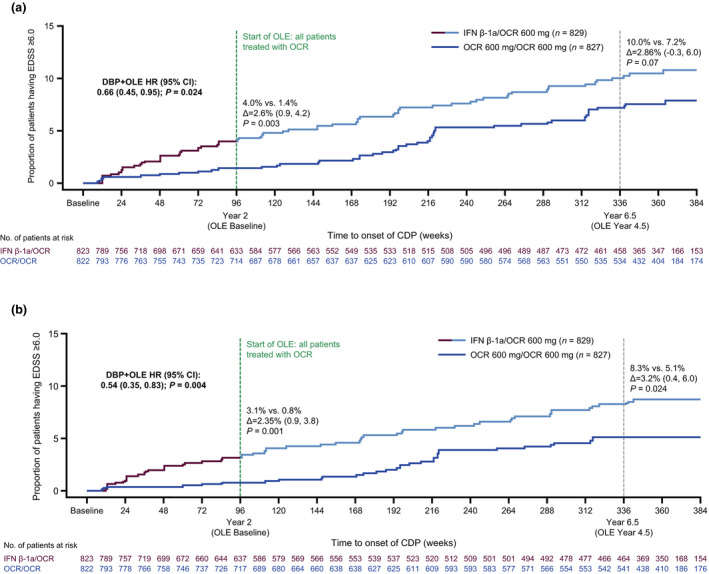
Methods: Time to EDSS score ≥6.0 confirmed for ≥24 and ≥48 weeks was assessed over the course of 6.5 years (336 weeks) in the double-blind period (DBP) and open-label extension (OLE) period of the OPERA I (NCT01247324) and OPERA II (NCT01412333) studies.
Results: Time to reach EDSS score ≥6.0 was significantly delayed in those initially randomized to OCR versus interferon. Over 6.5 years, the risk of requiring a walking aid confirmed for ≥24 weeks was 34% lower among those who initiated OCR earlier versus delayed treatment (average hazard ratio [HR] DBP + OLE 0.66, 95% confidence interval [CI] 0.45-0.95; p = 0.024); the risk of requiring a walking aid confirmed for ≥48 weeks was 46% lower (average HR DBP+OLE 0.54, 95% CI 0.35-0.83; p = 0.004).
Conclusion: The reduced risk of requiring a walking aid in earlier initiators of OCR demonstrates the long-term implications of earlier highly effective treatment.
Keywords: disease progression; interferon beta 1a; multiple sclerosis; ocrelizumab; walking stick.
© 2021 The Authors. European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
Figures
References
-
- Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983;33(11):1444‐1452. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
