

Characterization of genetics in patients with mucosal melanoma treated with immune checkpoint blockade
- PMID: 33724703
- PMCID: PMC8026918
- DOI: 10.1002/cam4.3789
Characterization of genetics in patients with mucosal melanoma treated with immune checkpoint blockade
Abstract
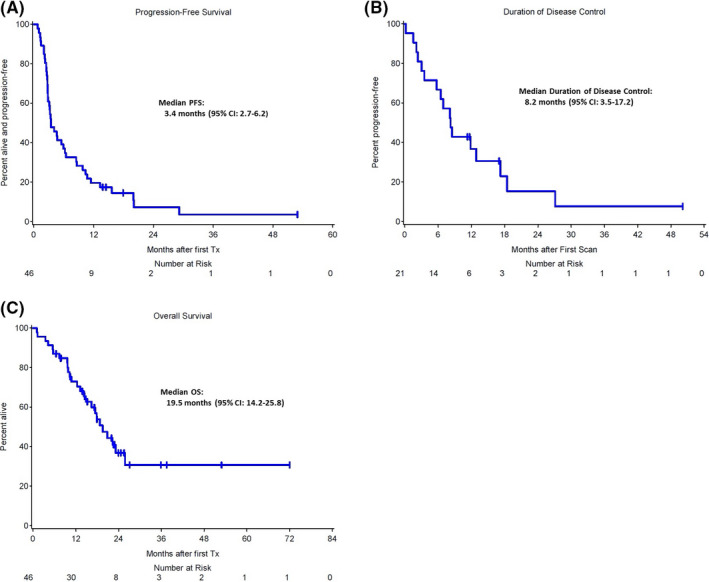
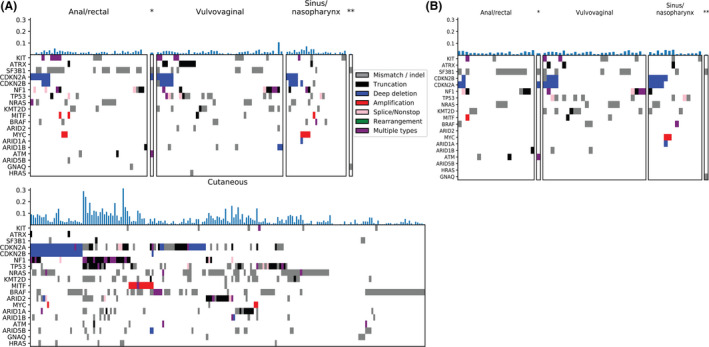
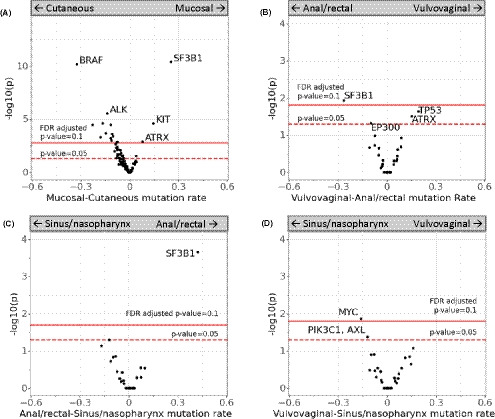
Mucosal melanoma is a rare form of melanoma which arises from melanocytes in the mucosal membranes and can be effectively treated with immune checkpoint blockade (ICB). However, response rates in mucosal melanoma are lower than those observed for cutaneous melanomas. Targeted sequencing of up to 447 genes (OncoPanel) was performed on tumors from all mucosal melanoma patients seen at the Dana-Farber Cancer Institute from 2011 until March 2019. We identified a total of 46 patients who received ICB with both tumor-genotype and ICB response data available. Within this cohort of patients, 16 (35%) had durable clinical benefit (DCB) to their first line of ICB. The average mutational burden/megabase was 6.23 and did not correlate with tumor response to ICB. Patients with KIT aberrations had a higher DCB rate compared with patients with wildtype KIT (71 vs. 28%), but this was not found to be statistically significant. For comparison, we analyzed tumor genotypes from an additional 50 mucosal melanoma tumors and 189 cutaneous melanoma tumors. The most frequent mutations in mucosal melanoma were in SF3B1 (27%), KIT (18%), and NF1 (17%), a pattern that is distinct from cutaneous melanomas. In addition, there were genetic differences observed based upon the site of origin of the mucosal melanoma. Our findings explore clinical features of response in patients with mucosal melanoma treated with ICB and demonstrate a low mutational burden that does not correlate with response. In addition, the lack of significant association between the genetic aberrations tested and response to ICB indicates the need for further exploration in this patient population.
Keywords: KIT mutation; genetics; immune checkpoint blockade; immunotherapy; mucosal melanoma.
© 2021 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
EB has served on advisory boards for Array Biopharma, Bristol‐Myers Squibb (BMS), Trieza Therapeutics and Novartis, and she also receives clinical trial support from Eli Lilly, Novartis, BMS, Genentech, and BVD. PAO reports the following: advisory roles for Alexion, Array, BMS, Celldex, CytomX, Genentech, Merck, Neon Therapeutics, Novartis, Pfizer, and TRM Oncology; institutional grants from Armo Biosciences, AstraZeneca/MedImmune, BMS, Celldex, CytomX, Genentech, Merck, Neon Therapeutics, Novartis, and Pfizer; and a speaking engagement from Medscape. SH reports the following: grants from BMS and Novartis; personal fees from BMS, Merck, Serono, Novartis, Takeda, Surface Pharmaceuticals, Genentech/Roche, Compass Therapeutics, Apricity, Bayer, Aduro, Partners Therapeutics, Sanofi, Pfizer, Pionyr Immunotherapeutics, 7 Hills Pharma, Verastem Oncology, Rheos Medicines, and Kairos Therapeutics; equity in Torque Therapeutics; and patents #20100111973 and #7250291 issued as well as #20170248603, #20160340407, #20160046716, #20140004112, #20170022275, #20170008962, and “Methods of Using Pembrolizumab and Trebananib” pending. L. Sholl‐ honorarium from Astra Zeneca; consulting income from EMD Serono; research grant funding from Roche/Genentech.
Figures

Similar articles
-
Whole-exome sequencing identifies recurrent SF3B1 R625 mutation and comutation of NF1 and KIT in mucosal melanoma.Melanoma Res. 2017 Jun;27(3):189-199. doi: 10.1097/CMR.0000000000000345. Melanoma Res. 2017. PMID: 28296713 Free PMC article.
-
The mutational landscape of mucosal melanoma.Semin Cancer Biol. 2020 Apr;61:139-148. doi: 10.1016/j.semcancer.2019.09.013. Epub 2019 Oct 23. Semin Cancer Biol. 2020. PMID: 31655118 Free PMC article. Review.
-
Targeted next generation sequencing of mucosal melanomas identifies frequent NF1 and RAS mutations.Oncotarget. 2017 Jun 20;8(25):40683-40692. doi: 10.18632/oncotarget.16542. Oncotarget. 2017. PMID: 28380455 Free PMC article.
-
NF1-mutated melanomas reveal distinct clinical characteristics depending on tumour origin and respond favourably to immune checkpoint inhibitors.Eur J Cancer. 2021 Dec;159:113-124. doi: 10.1016/j.ejca.2021.09.035. Epub 2021 Nov 4. Eur J Cancer. 2021. PMID: 34742158 Free PMC article.
-
Integrated genomic analysis identifies a genetic mutation model predicting response to immune checkpoint inhibitors in melanoma.Cancer Med. 2020 Nov;9(22):8498-8518. doi: 10.1002/cam4.3481. Epub 2020 Sep 24. Cancer Med. 2020. PMID: 32969604 Free PMC article.
Cited by
-
Primary Mucosal Melanoma: Clinical Experience from a Single Italian Center.Curr Oncol. 2024 Jan 22;31(1):588-597. doi: 10.3390/curroncol31010042. Curr Oncol. 2024. PMID: 38275835 Free PMC article.
-
Specific oncogene activation of the cell of origin in mucosal melanoma.bioRxiv [Preprint]. 2024 Apr 26:2024.04.22.590595. doi: 10.1101/2024.04.22.590595. bioRxiv. 2024. Update in: Nat Commun. 2025 Jul 22;16(1):6750. doi: 10.1038/s41467-025-61937-1. PMID: 38712250 Free PMC article. Updated. Preprint.
-
RAS pathway regulation in melanoma.Dis Model Mech. 2022 Feb 1;15(2):dmm049229. doi: 10.1242/dmm.049229. Epub 2022 Mar 2. Dis Model Mech. 2022. PMID: 35234863 Free PMC article. Review.
-
Clinical significance of genetic profiling based on different anatomic sites in patients with mucosal melanoma who received or did not receive immune checkpoint inhibitors.Cancer Cell Int. 2023 Aug 30;23(1):187. doi: 10.1186/s12935-023-03032-3. Cancer Cell Int. 2023. PMID: 37649078 Free PMC article.
-
Comparison of Prognostic Factors for Merkel Cell Carcinoma, Mucosal Melanoma and Cutaneous Malignant Melanoma: Insights into Their Etiologies.Curr Oncol. 2023 Mar 31;30(4):3974-3988. doi: 10.3390/curroncol30040301. Curr Oncol. 2023. PMID: 37185414 Free PMC article.
References
-
- Robert C, Long GV, Brady B, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med. 2015;372(4):320‐330. - PubMed
-
- Batsakis JG, Suarez P. Mucosal melanomas: a review. Adv Anat Pathol. 2000;7(3):167‐180. - PubMed
-
- Tomicic J, Wanebo HJ. Mucosal melanomas. Surg Clin North Am. 2003;83(2):237‐252. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
