

A Transcriptomic Signature for Risk-Stratification and Recurrence Prediction in Intrahepatic Cholangiocarcinoma
- PMID: 33725402
- PMCID: PMC8443691
- DOI: 10.1002/hep.31803
A Transcriptomic Signature for Risk-Stratification and Recurrence Prediction in Intrahepatic Cholangiocarcinoma
Abstract
Background and aims: Tumor recurrence is frequent even in intrahepatic cholangiocarcinoma (ICC), and improved strategies are needed to identify patients at highest risk for such recurrence. We performed genome-wide expression profile analyses to discover and validate a gene signature associated with recurrence in patients with ICC.
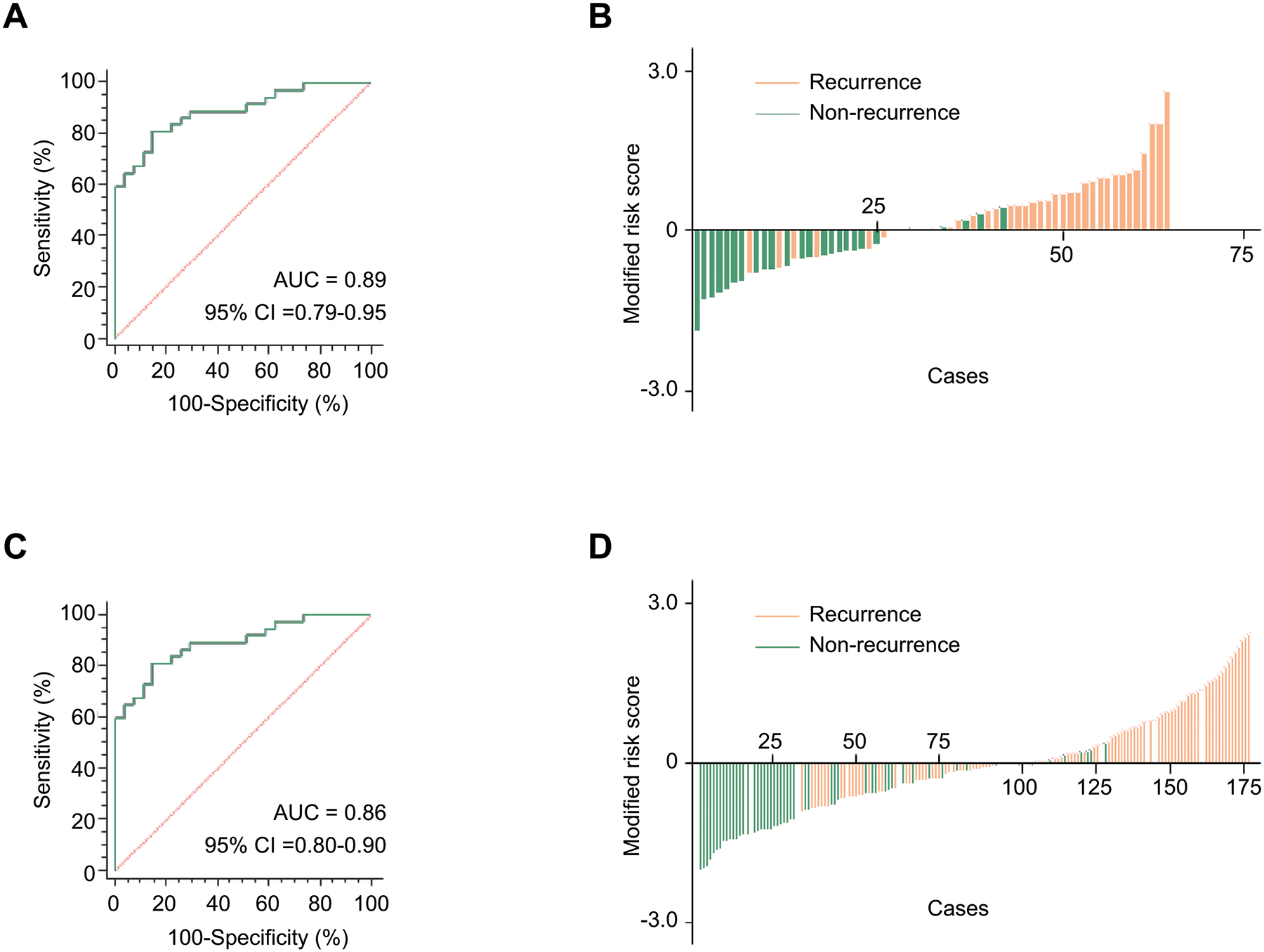
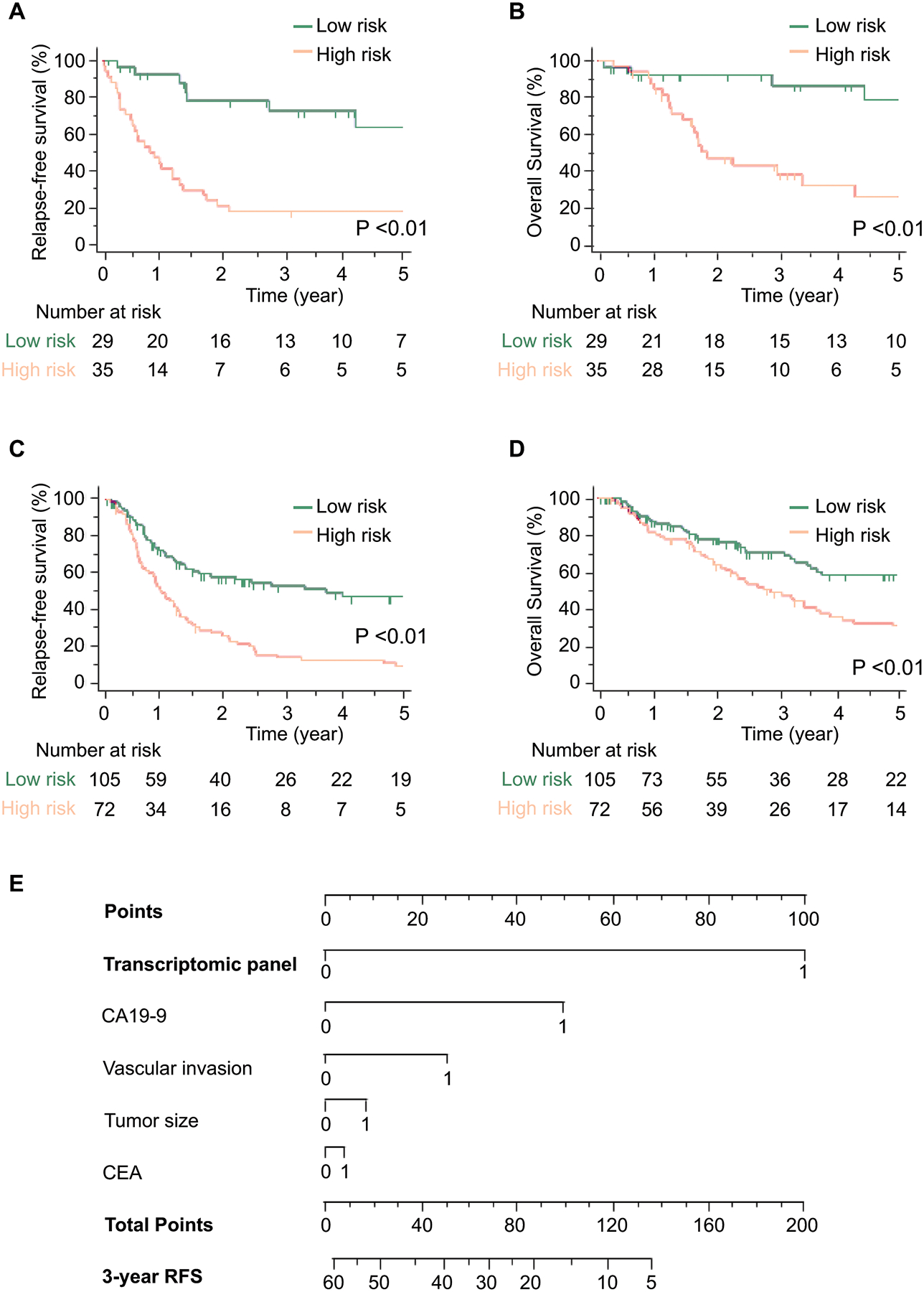
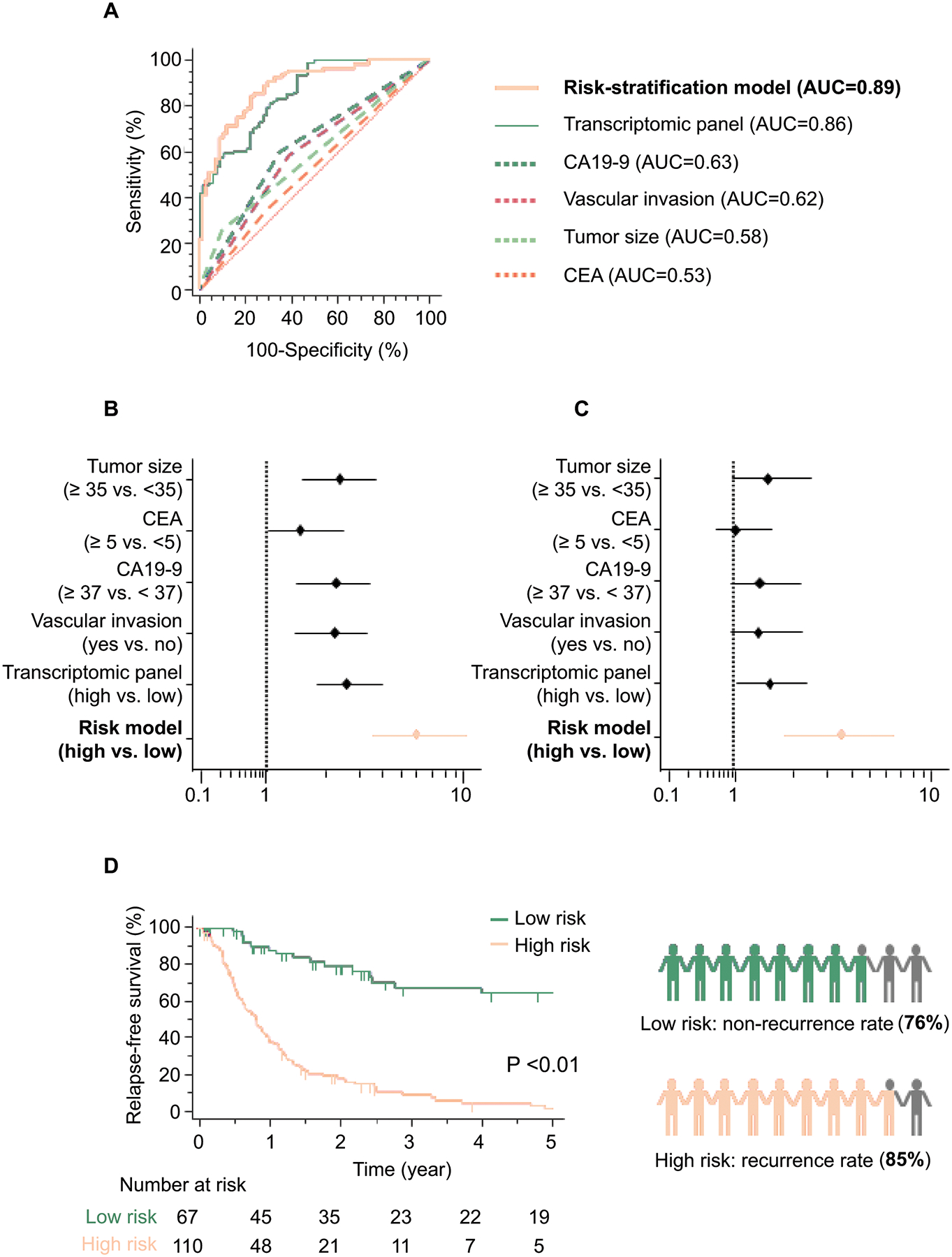
Approach and results: For biomarker discovery, we analyzed genome-wide transcriptomic profiling in ICC tumors from two public data sets: The Cancer Genome Atlas (n = 27) and GSE107943 (n = 28). We identified an eight-gene panel (BIRC5 [baculoviral IAP repeat containing 5], CDC20 [cell division cycle 20], CDH2 [cadherin 2], CENPW [centromere protein W], JPH1 [junctophilin 1], MAD2L1 [mitotic arrest deficient 2 like 1], NEIL3 [Nei like DNA glycosylase 3], and POC1A [POC1 centriolar protein A]) that robustly identified patients with recurrence in the discovery (AUC = 0.92) and in silico validation cohorts (AUC = 0.91). We next analyzed 241 specimens from patients with ICC (training cohort, n = 64; validation cohort, n = 177), followed by Cox proportional hazard regression analysis, to develop an integrated transcriptomic panel and establish a risk-stratification model for recurrence in ICC. We subsequently trained this transcriptomic panel in a clinical cohort (AUC = 0.89; 95% confidence interval [CI] = 0.79-0.95), followed by evaluating its performance in an independent validation cohort (AUC = 0.86; 95% CI = 0.80-0.90). By combining our transcriptomic panel with various clinicopathologic features, we established a risk-stratification model that was significantly superior for the identification of recurrence (AUC = 0.89; univariate HR = 6.08, 95% CI = 3.55-10.41, P < 0.01; and multivariate HR = 3.49, 95% CI = 1.81-6.71, P < 0.01). The risk-stratification model identified potential recurrence in 85% of high-risk patients and nonrecurrence in 76% of low-risk patients, which is dramatically superior to currently used pathological features.
Conclusions: We report a transcriptomic signature for risk-stratification and recurrence prediction that is superior to currently used clinicopathological features in patients with ICC.
© 2021 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Conflict of Interest: None of the authors has any potential conflicts to disclose.
Figures
References
-
- Aljiffry M, Abdulelah A, Walsh M, Peltekian K, Alwayn I, Molinari M. Evidence-based approach to cholangiocarcinoma: a systematic review of the current literature. J Am Coll Surg 2009;208:134–147. - PubMed
-
- Bertuccio P, Malvezzi M, Carioli G, Hashim D, Boffetta P, El-Serag HB, La Vecchia C, et al. Global trends in mortality from intrahepatic and extrahepatic cholangiocarcinoma. J Hepatol 2019;71:104–114. - PubMed
-
- Khan SA, Thomas HC, Davidson BR, Taylor-Robinson SD. Cholangiocarcinoma. Lancet 2005;366:1303–1314. - PubMed
-
- Mavros MN, Economopoulos KP, Alexiou VG, Pawlik TM. Treatment and Prognosis for Patients With Intrahepatic Cholangiocarcinoma: Systematic Review and Meta-analysis. JAMA Surg 2014;149:565–574. - PubMed
-
- Amini N, Ejaz A, Spolverato G, Kim Y, Herman JM, Pawlik TM. Temporal trends in liver-directed therapy of patients with intrahepatic cholangiocarcinoma in the United States: a population-based analysis. J Surg Oncol 2014;110:163–170. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
