

Efficacy of Early (≤ 24 Hours), Late (25-72 Hours), and Delayed (>72 Hours) Surgery with Magnetic Resonance Imaging-Confirmed Decompression in American Spinal Injury Association Impairment Scale Grades C and D Acute Traumatic Central Cord Syndrome Caused by Spinal Stenosis
- PMID: 33726507
- PMCID: PMC8309437
- DOI: 10.1089/neu.2021.0040
Efficacy of Early (≤ 24 Hours), Late (25-72 Hours), and Delayed (>72 Hours) Surgery with Magnetic Resonance Imaging-Confirmed Decompression in American Spinal Injury Association Impairment Scale Grades C and D Acute Traumatic Central Cord Syndrome Caused by Spinal Stenosis
Abstract
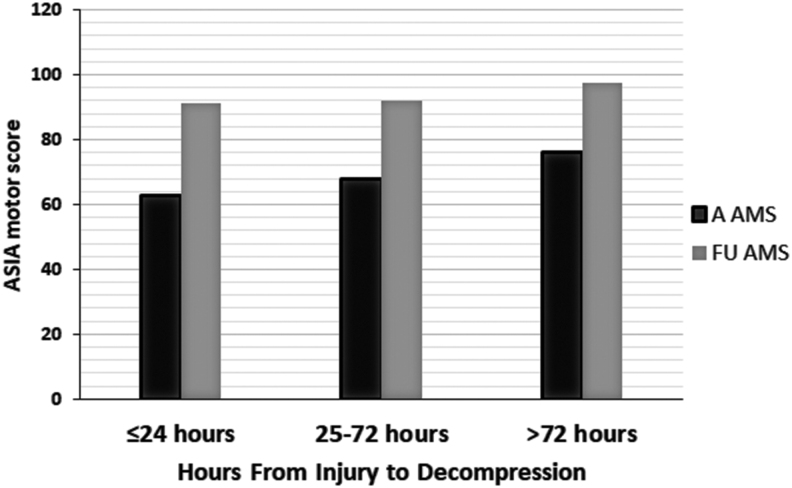
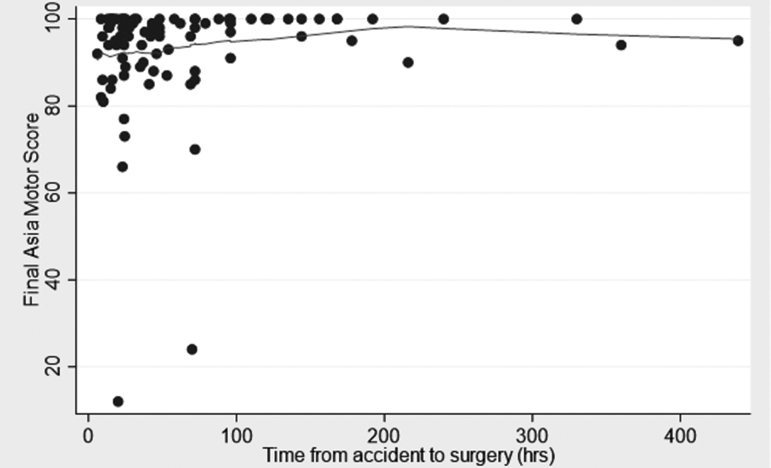
The therapeutic significance of timing of decompression in acute traumatic central cord syndrome (ATCCS) caused by spinal stenosis remains unsettled. We retrospectively examined a homogenous cohort of patients with ATCCS and magnetic resonance imaging (MRI) evidence of post-treatment spinal cord decompression to determine whether timing of decompression played a significant role in American Spinal Injury Association (ASIA) motor score (AMS) 6 months following trauma. We used the t test, analysis of variance, Pearson correlation coefficient, and multiple regression for statistical analysis. During a 19-year period, 101 patients with ATCCS, admission ASIA Impairment Scale (AIS) grades C and D, and an admission AMS of ≤95 were surgically decompressed. Twenty-four of 101 patients had an AIS grade C injury. Eighty-two patients were males, the mean age of patients was 57.9 years, and 69 patients had had a fall. AMS at admission was 68.3 (standard deviation [SD] 23.4); upper extremities (UE) 28.6 (SD 14.7), and lower extremities (LE) 41.0 (SD 12.7). AMS at the latest follow-up was 93.1 (SD 12.8), UE 45.4 (SD 7.6), and LE 47.9 (SD 6.6). Mean number of stenotic segments was 2.8, mean canal compromise was 38.6% (SD 8.7%), and mean intramedullary lesion length (IMLL) was 23 mm (SD 11). Thirty-six of 101 patients had decompression within 24 h, 38 patients had decompression between 25 and 72 h, and 27 patients had decompression >72 h after injury. Demographics, etiology, AMS, AIS grade, morphometry, lesion length, surgical technique, steroid protocol, and follow-up AMS were not statistically different between groups treated at different times. We analyzed the effect size of timing of decompression categorically and in a continuous fashion. There was no significant effect of the timing of decompression on follow-up AMS. Only AMS at admission determined AMS at follow-up (coefficient = 0.31; 95% confidence interval [CI]:0.21; p = 0.001). We conclude that timing of decompression in ATCCS caused by spinal stenosis has little bearing on ultimate AMS at follow-up.
Keywords: decompression; outcome; spinal cord injury; timing; trauma.
Conflict of interest statement
No competing financial interests exist.
Figures
Similar articles
-
Efficacy of Ultra-Early (< 12 h), Early (12-24 h), and Late (>24-138.5 h) Surgery with Magnetic Resonance Imaging-Confirmed Decompression in American Spinal Injury Association Impairment Scale Grades A, B, and C Cervical Spinal Cord Injury.J Neurotrauma. 2020 Feb 1;37(3):448-457. doi: 10.1089/neu.2019.6606. Epub 2019 Aug 1. J Neurotrauma. 2020. PMID: 31310155 Free PMC article.
-
Predictors of outcome in acute traumatic central cord syndrome due to spinal stenosis.J Neurosurg Spine. 2011 Jan;14(1):122-30. doi: 10.3171/2010.9.SPINE09922. Epub 2010 Dec 17. J Neurosurg Spine. 2011. PMID: 21166485
-
Predicting the Role of Preoperative Intramedullary Lesion Length and Early Decompressive Surgery in ASIA Impairment Scale Grade Improvement Following Subaxial Traumatic Cervical Spinal Cord Injury.J Neurol Surg A Cent Eur Neurosurg. 2023 Mar;84(2):144-156. doi: 10.1055/s-0041-1740379. Epub 2022 Jun 3. J Neurol Surg A Cent Eur Neurosurg. 2023. PMID: 35668673 Free PMC article.
-
Acute traumatic central cord syndrome: a comprehensive review.Neurochirurgie. 2014 Feb-Apr;60(1-2):5-11. doi: 10.1016/j.neuchi.2013.12.002. Epub 2014 Mar 7. Neurochirurgie. 2014. PMID: 24613283 Review.
-
Surgical intervention ≤ 24 hours versus > 24 hours after injury for the management of acute traumatic central cord syndrome: a systematic review and meta-analysis.J Neurosurg Spine. 2024 Feb 9;40(5):653-661. doi: 10.3171/2023.11.SPINE23789. Print 2024 May 1. J Neurosurg Spine. 2024. PMID: 38335527
Cited by
-
Time from injury to acute surgery for patients with traumatic cervical spinal cord injury in South-East Norway.Front Neurol. 2024 Jun 24;15:1420530. doi: 10.3389/fneur.2024.1420530. eCollection 2024. Front Neurol. 2024. PMID: 38978812 Free PMC article.
-
Pathophysiology and surgical decision-making in central cord syndrome and degenerative cervical myelopathy: correcting the somatotopic fallacy.Front Neurol. 2023 Nov 17;14:1276399. doi: 10.3389/fneur.2023.1276399. eCollection 2023. Front Neurol. 2023. PMID: 38046579 Free PMC article. Review.
-
[Risk factors associated with lethality on patients with central cord syndrome].Rev Med Inst Mex Seguro Soc. 2023 Oct 2;61(Suppl 3):S437-S444. doi: 10.5281/zenodo.8319828. Rev Med Inst Mex Seguro Soc. 2023. PMID: 37934901 Free PMC article. Spanish.
-
Spinal cord injury: Current trends in acute management.Brain Spine. 2024 Apr 7;4:102803. doi: 10.1016/j.bas.2024.102803. eCollection 2024. Brain Spine. 2024. PMID: 38618228 Free PMC article. Review.
-
Time is spine: What's over the horizon.J Clin Orthop Trauma. 2022 Oct 22;35:102043. doi: 10.1016/j.jcot.2022.102043. eCollection 2022 Dec. J Clin Orthop Trauma. 2022. PMID: 36340959 Free PMC article.
References
-
- Schneider, R.C. (1951). A syndrome in acute cervical spine injuries for which early operation is indicated. J. Neurosurg. 8, 360–367 - PubMed
-
- Schneider, R.C., Cherry, G., and Pantek, H. (1954). The syndrome of acute central cervical spinal cord injury. J. Neurosurg. 13, 546–577 - PubMed
-
- Schneider, R.C., Crosby, E.C., Russo, R.H., and Gosch, H.H. (1973). Traumatic spinal cord syndromes and their management. Clin. Neurosurg. 20, 424–492 - PubMed
-
- Yoshihara, H., and Yoneoka, D. (2013). Trends in the treatment for traumatic central cord syndrome without bone injury in the United States from 2000 to 2009. J. Trauma Acute Care Surg. 75, 453–458 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical