

The influence of powered prostheses on user perspectives, metabolics, and activity: a randomized crossover trial
- PMID: 33726802
- PMCID: PMC7962267
- DOI: 10.1186/s12984-021-00842-2
The influence of powered prostheses on user perspectives, metabolics, and activity: a randomized crossover trial
Abstract
Background: Powered prosthetic ankles provide battery-powered mechanical push-off, with the aim of reducing the metabolic demands of walking for people with transtibial amputations. The efficacy of powered ankles has been shown in active, high functioning individuals with transtibial amputation, but is less clear in other populations. Additionally, it is unclear how use of a powered prosthesis influences everyday physical activity and mobility.
Methods: Individuals with unilateral transtibial amputations participated in a randomized clinical trial comparing their prescribed, unpowered prosthesis and the BiOM powered prosthesis. Participants' metabolic costs and self-selected walking speeds were measured in the laboratory and daily step count, daily steps away from home, and walking speed were measured over two weeks of at-home prosthesis use. Participants also rated their perception of mobility and quality of life and provided free-form feedback. Dependent measures were compared between prostheses and the relationships between metabolic cost, perception of mobility, and characteristics of walking in daily life were explored using Pearson's correlations.
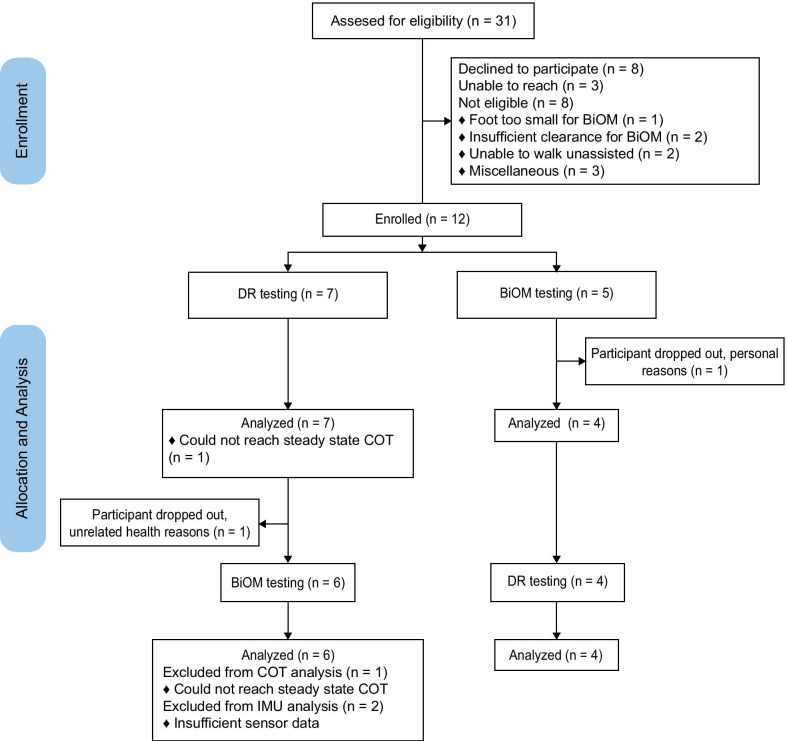
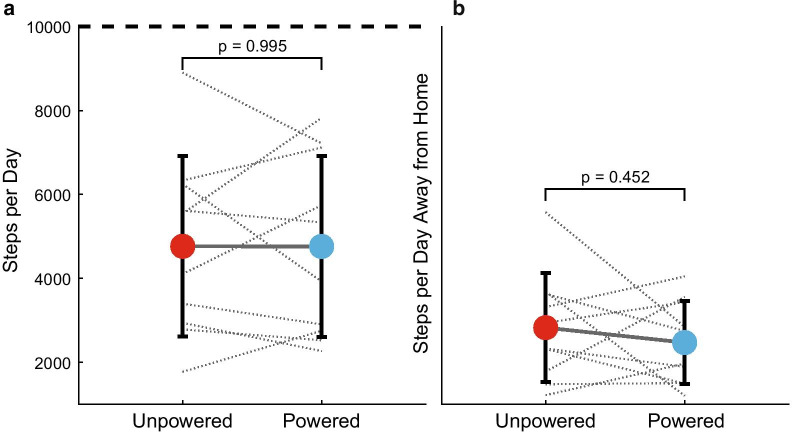
Results: Twelve people were randomly allocated to the powered prosthesis first (n = 7) or unpowered prosthesis first (n = 5) and ten completed the full study. There were no differences in metabolic costs (p = 0.585), daily step count (p = 0.995), walking speed in-lab (p = 0.145) and in daily life (p = 0.226), or perception of mobility between prostheses (p ≥ 0.058). Changes varied across participants, however. There were several medium-sized effects for device comparisons. With the powered prosthesis, participants had increased self-reported ambulation (g = 0.682) and decreased frustration (g = 0.506).
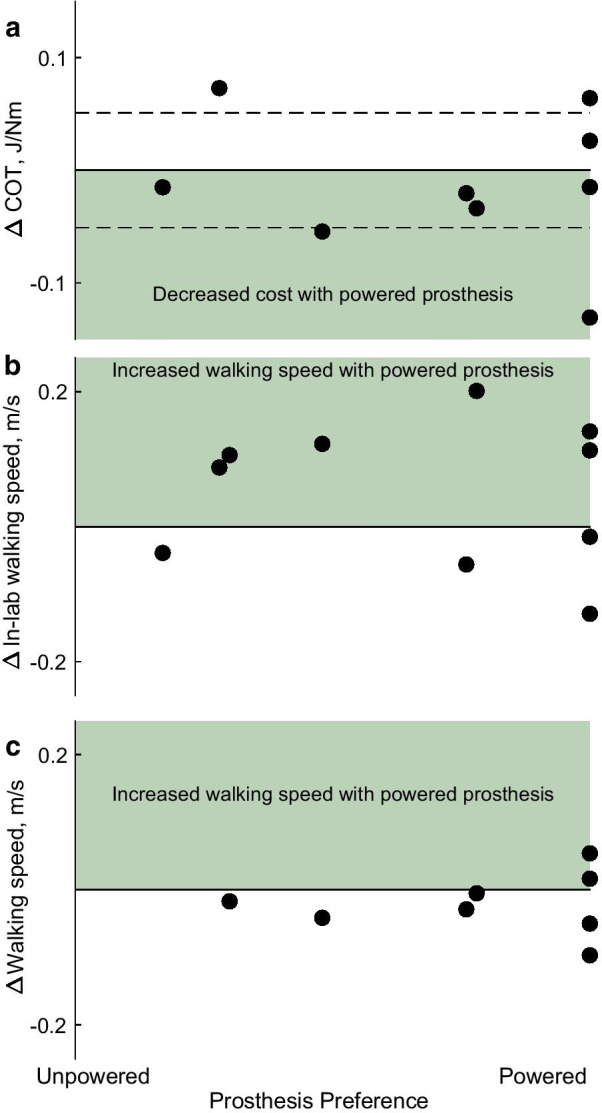
Conclusions: There were no universal benefits of the powered prosthesis on function in the lab or home environment. However, the effects were subject-specific, with some reporting preference for power and improved mobility, and some increasing their activity and decreasing their metabolic effort. Additionally, self-reported preferences did not often correlate with objective measures of function. This highlights the need for future clinical research to include both perception and objective measures to better inform prosthetic prescription.
Trial registration: https://clinicaltrials.gov , #NCT02828982. Registered 12 July 2016, https://clinicaltrials.gov/ct2/show/NCT02828982.
Keywords: Accelerometer; Inertial measurement unit; Metabolic cost; Microprocessor ankle; Preference; Step count; Transtibial amputation; Walking speed.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
