

Targeted next-generation sequencing supports serrated epithelial change as an early precursor to inflammatory bowel disease-associated colorectal neoplasia
- PMID: 33727167
- PMCID: PMC10113803
- DOI: 10.1016/j.humpath.2021.03.002
Targeted next-generation sequencing supports serrated epithelial change as an early precursor to inflammatory bowel disease-associated colorectal neoplasia
Abstract
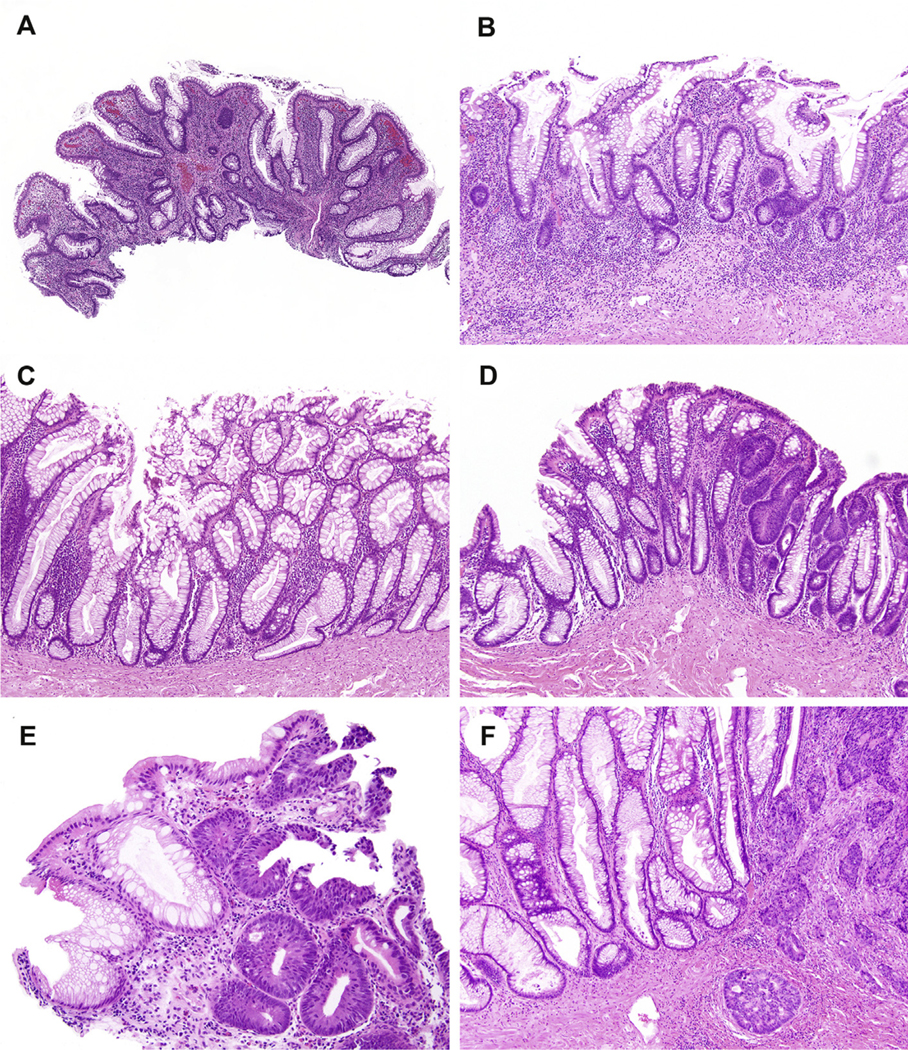
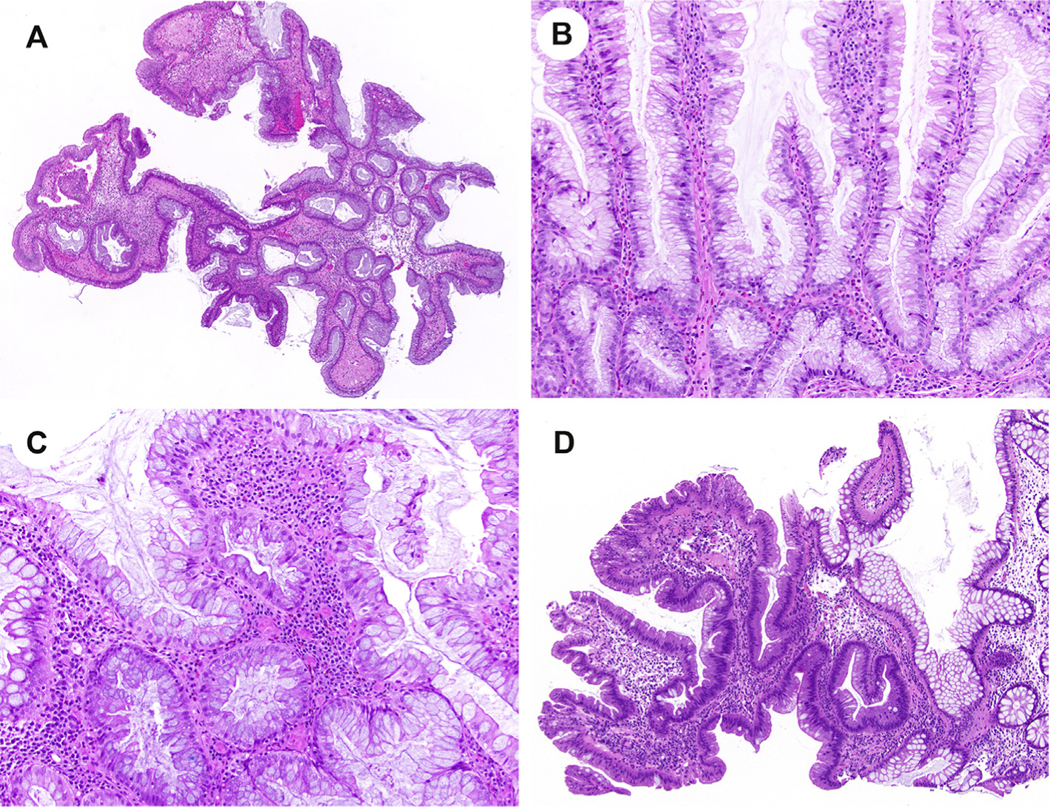
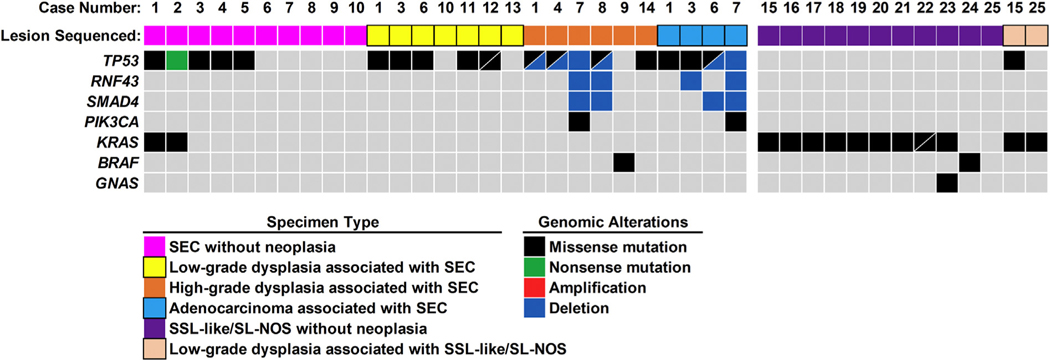
Serrated epithelial change (SEC) manifests in patients with long-standing inflammatory bowel disease (IBD) and is characterized by disorganized crypt architecture, irregular serrations, and goblet cell-rich epithelium. The serrated nature of SEC is reminiscent of serrated colorectal polyps, which frequently harbor KRAS/BRAF mutations. SEC is, however, not only histologically distinct from sporadic serrated polyps but also associated with colorectal neoplasia. Whether SEC is a precursor to IBD-associated neoplasia remains unclear. To further define the relationship of SEC with serrated colorectal polyps and IBD-associated neoplasia, we performed targeted next-generation sequencing on colorectal specimens to include the following: SEC without dysplasia/neoplasia (n = 10), SEC with separate foci of associated dysplasia/adenocarcinoma from the same patients (n = 17), and uninvolved mucosa (n = 10) from 14 patients. In addition, we molecularly profiled sessile serrated lesion (SSL)-like or serrated lesion, not otherwise specified (SL-NOS), specimens, from 11 patients who also had IBD. This control cohort included SSL-like/SL-NOS without dysplasia/neoplasia (n = 11), SSL-like/SL-NOS with associated low-grade dysplasia (n = 2), and uninvolved mucosa (n = 8). By next-generation sequencing, the most frequently mutated gene in SEC without neoplasia and associated dysplasia/adenocarcinoma from separate foci in the same patients was TP53. Recurrent TP53 mutations were present in 50% of SEC specimens without dysplasia/neoplasia. In addition, alterations in TP53 were detected at a prevalence of 71% in low-grade dysplasia, 83% in high-grade dysplasia, and 100% in adenocarcinoma. Paired sequencing of SEC and associated neoplasia revealed identical TP53 missense mutations for 3 patients. In contrast, 91% of SSL-like/SL-NOS specimens without dysplasia/neoplasia harbored KRAS/BRAF mutations, which were conserved in associated low-grade dysplasia. No genomic alterations were found in uninvolved mucosa from either patients with SEC or patients with SSL-like/SL-NOS. Based on our findings, we conclude SEC is distinct from SSL-like serrated colorectal lesions in patients with IBD and an early precursor to IBD-associated neoplasia that warrants colonoscopic surveillance.
Keywords: Colon cancer; Crohn disease; Hyperplastic polyp; Serrated dysplasia; Sessile serrated adenoma/lesion; Ulcerative colitis.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Competing interests: A.D.S. has received an honorarium from Foundation Medicine, Inc. The remaining authors have disclosed that they have no financial interests, arrangements, affiliations, or commercial interests with the manufacturers of any products discussed in this article or their competitors.
Figures
References
-
- Jess T, Gamborg M, Matzen P, Munkholm P, Sorensen TI. Increased risk of intestinal cancer in crohn’s disease: a meta-analysis of population-based cohort studies. Am J Gastroenterol 2005;100:2724–9. - PubMed
-
- Rutter MD, Saunders BP, Wilkinson KH, Rumbles S, Schofield G, Kamm MA, et al. Thirty-year analysis of a colonoscopic surveillance program for neoplasia in ulcerative colitis. Gastroenterology 2006;130:1030–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
