

Phase II Clinical Trial of Everolimus in a Pan-Cancer Cohort of Patients with mTOR Pathway Alterations
- PMID: 33727259
- PMCID: PMC8282751
- DOI: 10.1158/1078-0432.CCR-20-4548
Phase II Clinical Trial of Everolimus in a Pan-Cancer Cohort of Patients with mTOR Pathway Alterations
Abstract
Purpose: This was a multicenter, histology-agnostic, single-arm prospective phase II trial of therapeutic activity of everolimus, an oral mTORC1 inhibitor, in patients with advanced solid tumors that harbored TSC1/TSC2 or MTOR mutations.
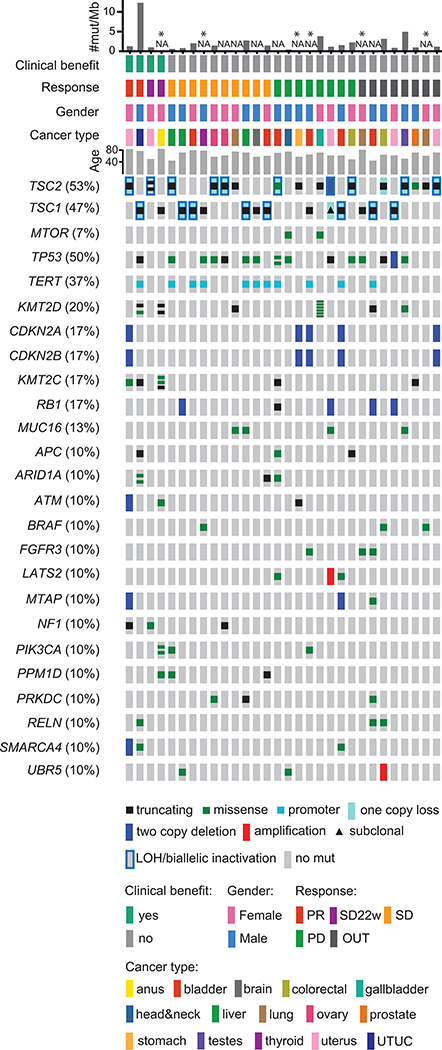
Patients and methods: Patients with tumors with inactivating TSC1/TSC2 or activating MTOR mutations identified in any Clinical Laboratory Improvement Amendments (CLIA)-certified laboratory were eligible. Patients were treated with everolimus 10 mg once daily until disease progression or unacceptable toxicity. The primary endpoint was objective response rate (ORR). Whole-exome sequencing was performed to identify co-occurring genomic alterations.
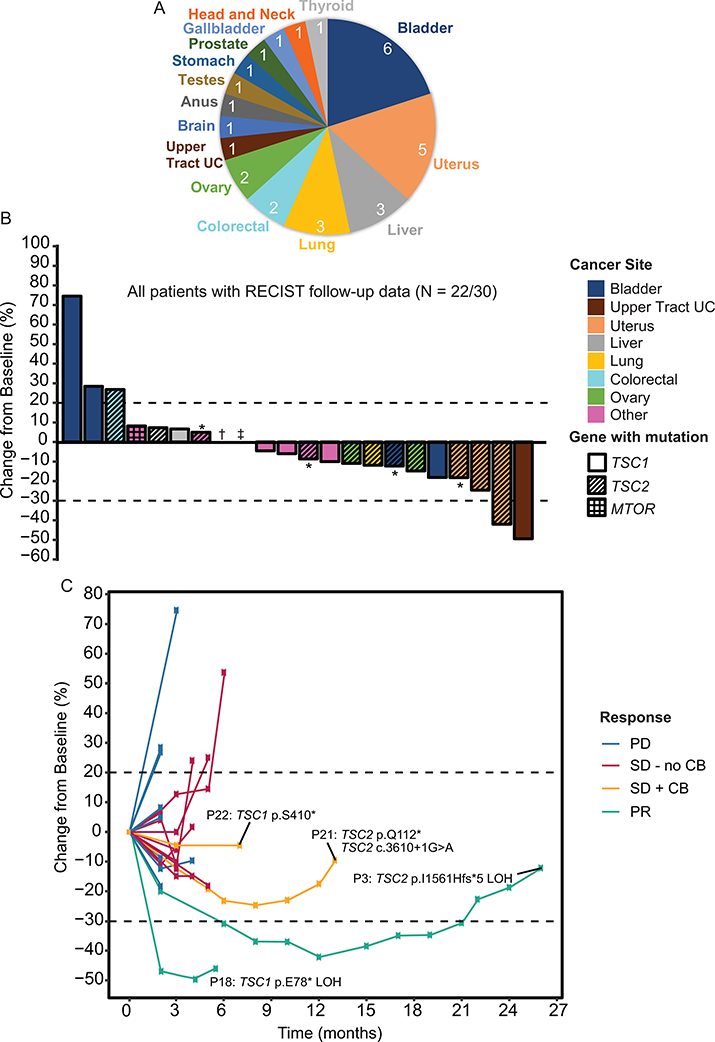
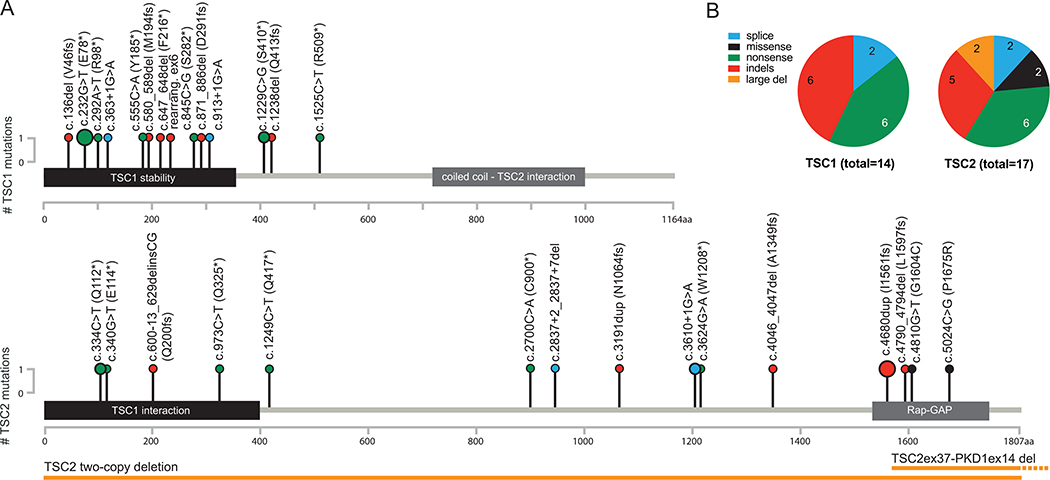
Results: Between November 2015 and October 2018, 30 patients were enrolled at Dana-Farber Cancer Institute and Memorial Sloan Kettering Cancer Center. Tumors harbored TSC1 (13/30), TSC2 (15/30), concurrent TSC1 and TSC2 (1/30), or MTOR (1/30) mutations. The most common treatment-related adverse event of any grade was mucositis (8/30, 27%); 1 patient had fatal pneumonitis. Partial responses were seen in 2 patients [7%; 95% confidence interval (CI), 1%-22%]. Median progression-free survival was 2.3 months (95% CI, 1.8-3.7 months) and median overall survival (OS) was 7.3 months (95% CI, 4.5-12.7 months). There was no clear association between other genomic alterations and response. Of the 2 patients with objective response, 1 had upper tract urothelial carcinoma with biallelic inactivation of TSC1 and high tumor mutation burden, and the other had uterine carcinoma with biallelic TSC2-inactivating mutations and PEComa-like pathologic features.
Conclusions: Everolimus therapy had a disappointing ORR (7%) in this pan-cancer, mutation-selected, basket study.See related commentary by Kato and Cohen, p. 3807.
©2021 American Association for Cancer Research.
Figures
Comment in
-
Did Everolimus Break the Rules?Clin Cancer Res. 2021 Jul 15;27(14):3807-3808. doi: 10.1158/1078-0432.CCR-21-1508. Epub 2021 May 13. Clin Cancer Res. 2021. PMID: 33986025
Similar articles
-
PTEN Expression, Not Mutation Status in TSC1, TSC2, or mTOR, Correlates with the Outcome on Everolimus in Patients with Renal Cell Carcinoma Treated on the Randomized RECORD-3 Trial.Clin Cancer Res. 2019 Jan 15;25(2):506-514. doi: 10.1158/1078-0432.CCR-18-1833. Epub 2018 Oct 16. Clin Cancer Res. 2019. PMID: 30327302 Clinical Trial.
-
Next-generation sequencing reveals somatic mutations that confer exceptional response to everolimus.Oncotarget. 2016 Mar 1;7(9):10547-56. doi: 10.18632/oncotarget.7234. Oncotarget. 2016. PMID: 26859683 Free PMC article.
-
PTEN expression and mutations in TSC1, TSC2 and MTOR are associated with response to rapalogs in patients with renal cell carcinoma.Int J Cancer. 2020 Mar 1;146(5):1435-1444. doi: 10.1002/ijc.32579. Epub 2019 Aug 9. Int J Cancer. 2020. PMID: 31335987
-
Everolimus in patients with metastatic renal cell carcinoma previously treated with bevacizumab: a prospective multicenter study CRAD001LRU02T.Target Oncol. 2015 Sep;10(3):423-7. doi: 10.1007/s11523-014-0347-4. Epub 2014 Dec 4. Target Oncol. 2015. PMID: 25466382 Clinical Trial.
-
Differentiating the mTOR inhibitors everolimus and sirolimus in the treatment of tuberous sclerosis complex.Neuro Oncol. 2015 Dec;17(12):1550-9. doi: 10.1093/neuonc/nov152. Epub 2015 Aug 19. Neuro Oncol. 2015. PMID: 26289591 Free PMC article. Review.
Cited by
-
Precision Medicine to Treat Urothelial Carcinoma-The Way Forward.Cancers (Basel). 2023 Jun 1;15(11):3024. doi: 10.3390/cancers15113024. Cancers (Basel). 2023. PMID: 37296985 Free PMC article. Review.
-
Inhibition of the AKT/mTOR pathway negatively regulates PTEN expression via miRNAs.Acta Biochim Biophys Sin (Shanghai). 2022 Oct 25;54(11):1637-1647. doi: 10.3724/abbs.2022159. Acta Biochim Biophys Sin (Shanghai). 2022. PMID: 36331296 Free PMC article.
-
Pifithrin-μ sensitizes mTOR-activated liver cancer to sorafenib treatment.Cell Death Dis. 2025 Jan 26;16(1):42. doi: 10.1038/s41419-025-07332-6. Cell Death Dis. 2025. PMID: 39863613 Free PMC article.
-
PI3K/AKT/mTOR Axis in Cancer: From Pathogenesis to Treatment.MedComm (2020). 2025 Jul 30;6(8):e70295. doi: 10.1002/mco2.70295. eCollection 2025 Aug. MedComm (2020). 2025. PMID: 40740483 Free PMC article. Review.
-
Bi-steric mTORC1 inhibitors induce apoptotic cell death in tumor models with hyperactivated mTORC1.J Clin Invest. 2023 Nov 1;133(21):e167861. doi: 10.1172/JCI167861. J Clin Invest. 2023. PMID: 37909334 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
