

Leukocyte Heterogeneity in Pancreatic Ductal Adenocarcinoma: Phenotypic and Spatial Features Associated with Clinical Outcome
- PMID: 33727309
- PMCID: PMC8338775
- DOI: 10.1158/2159-8290.CD-20-0841
Leukocyte Heterogeneity in Pancreatic Ductal Adenocarcinoma: Phenotypic and Spatial Features Associated with Clinical Outcome
Abstract
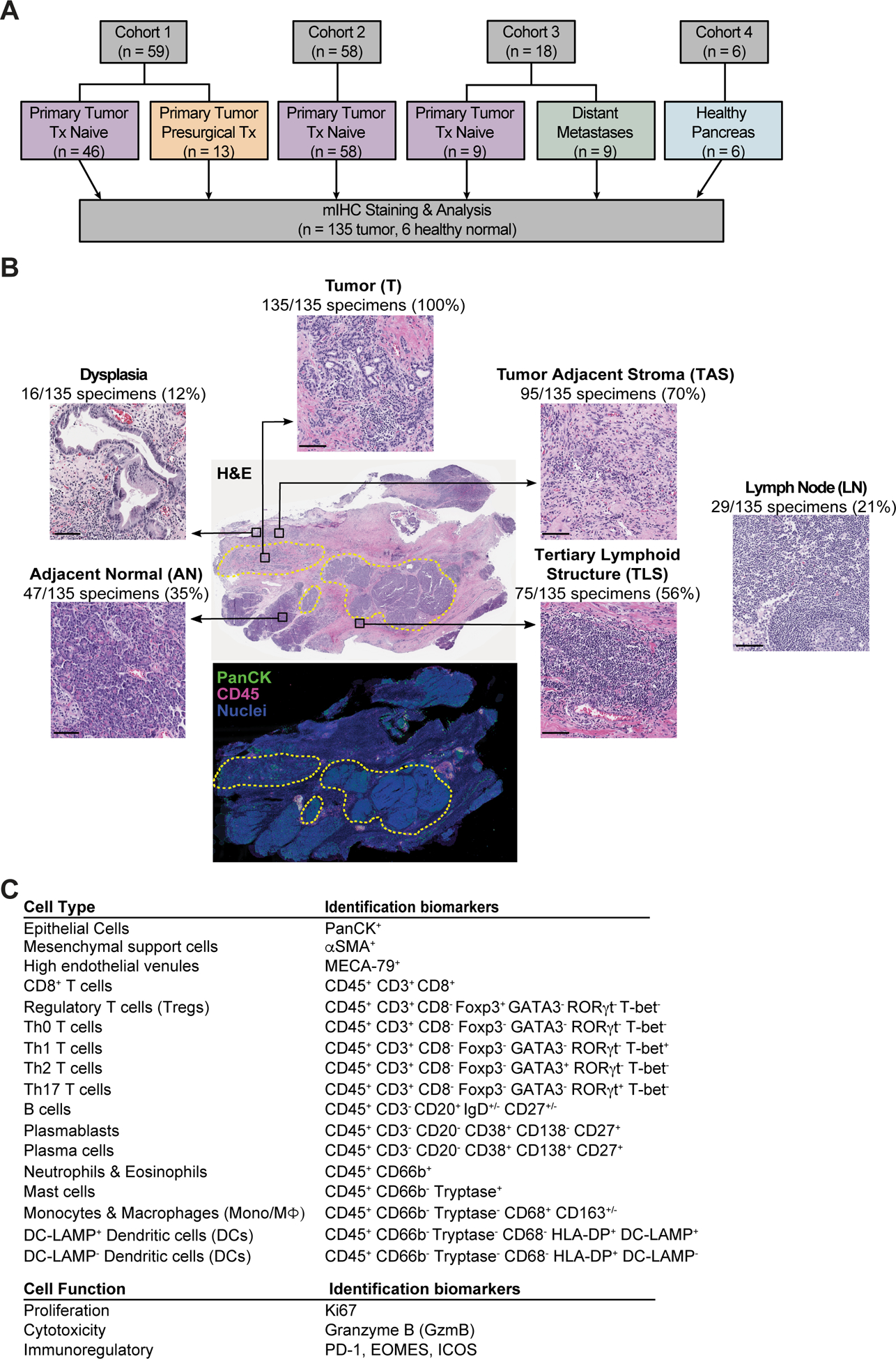
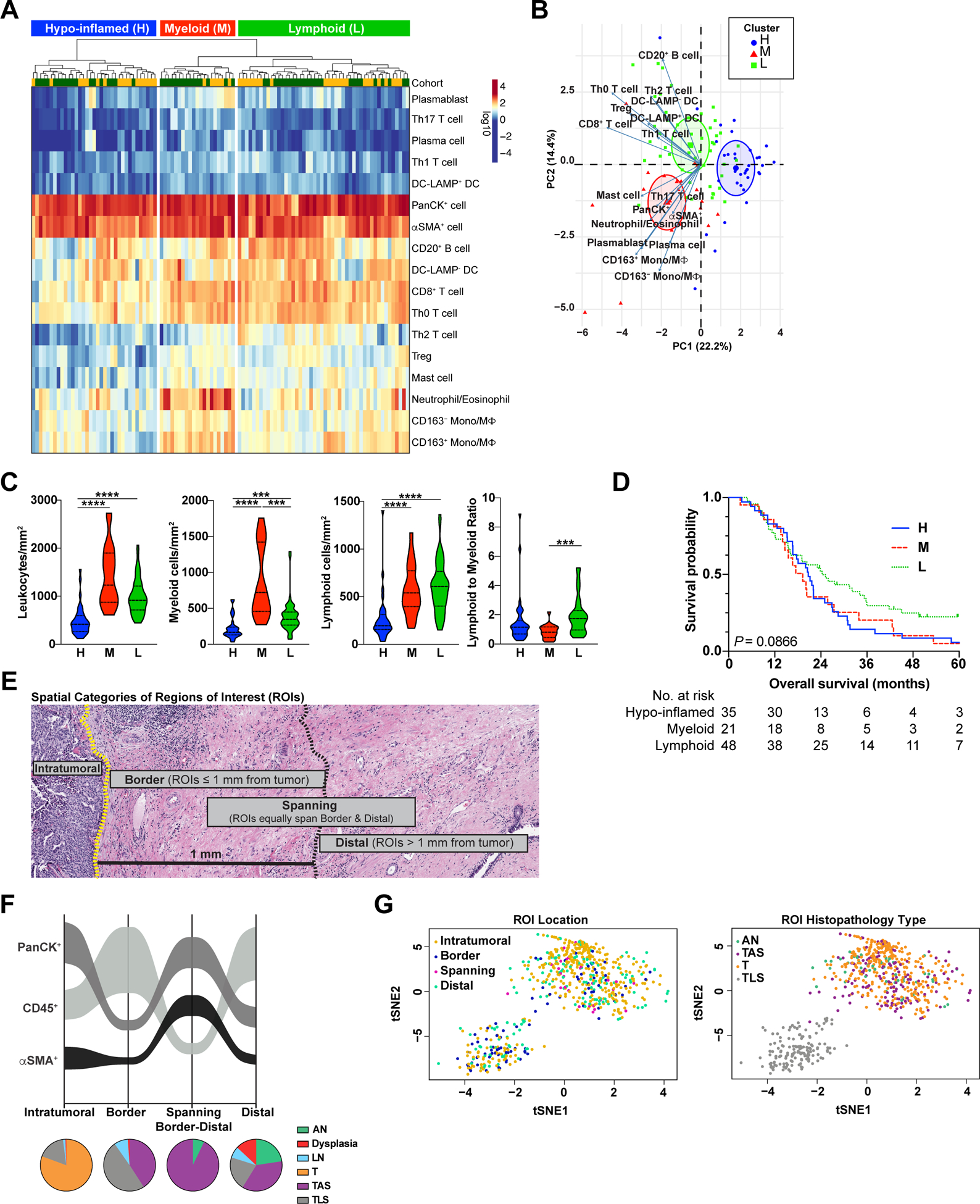
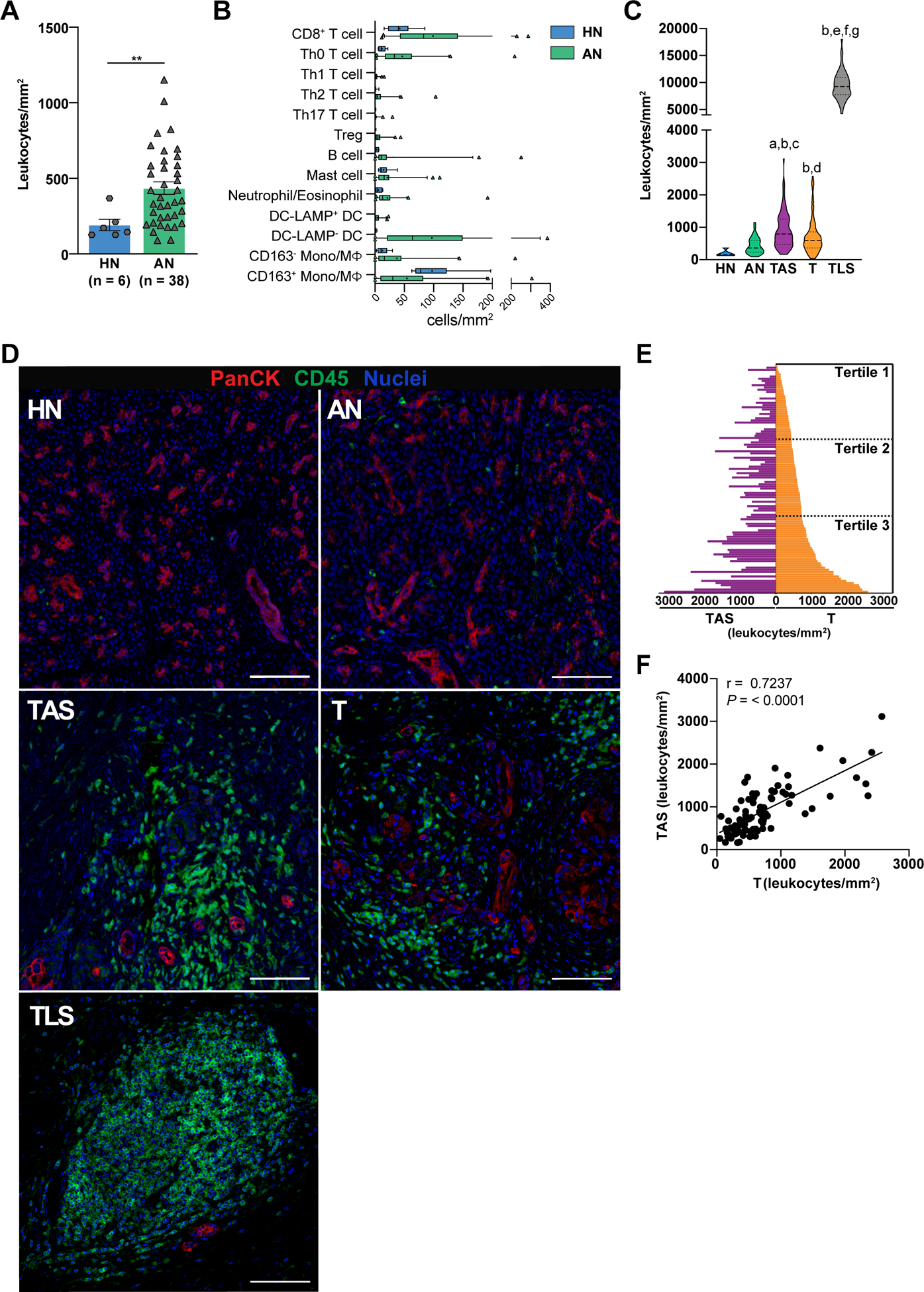
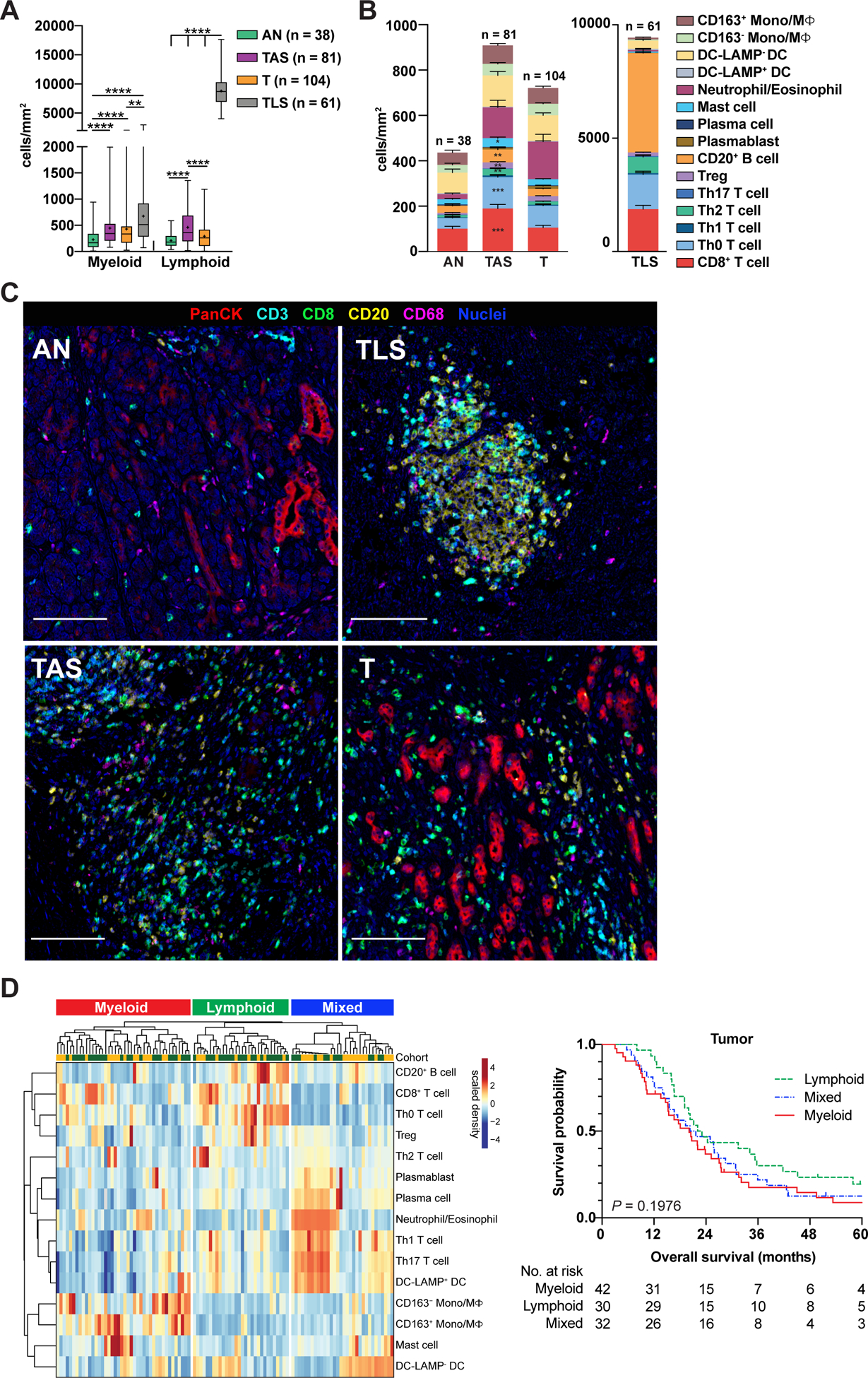
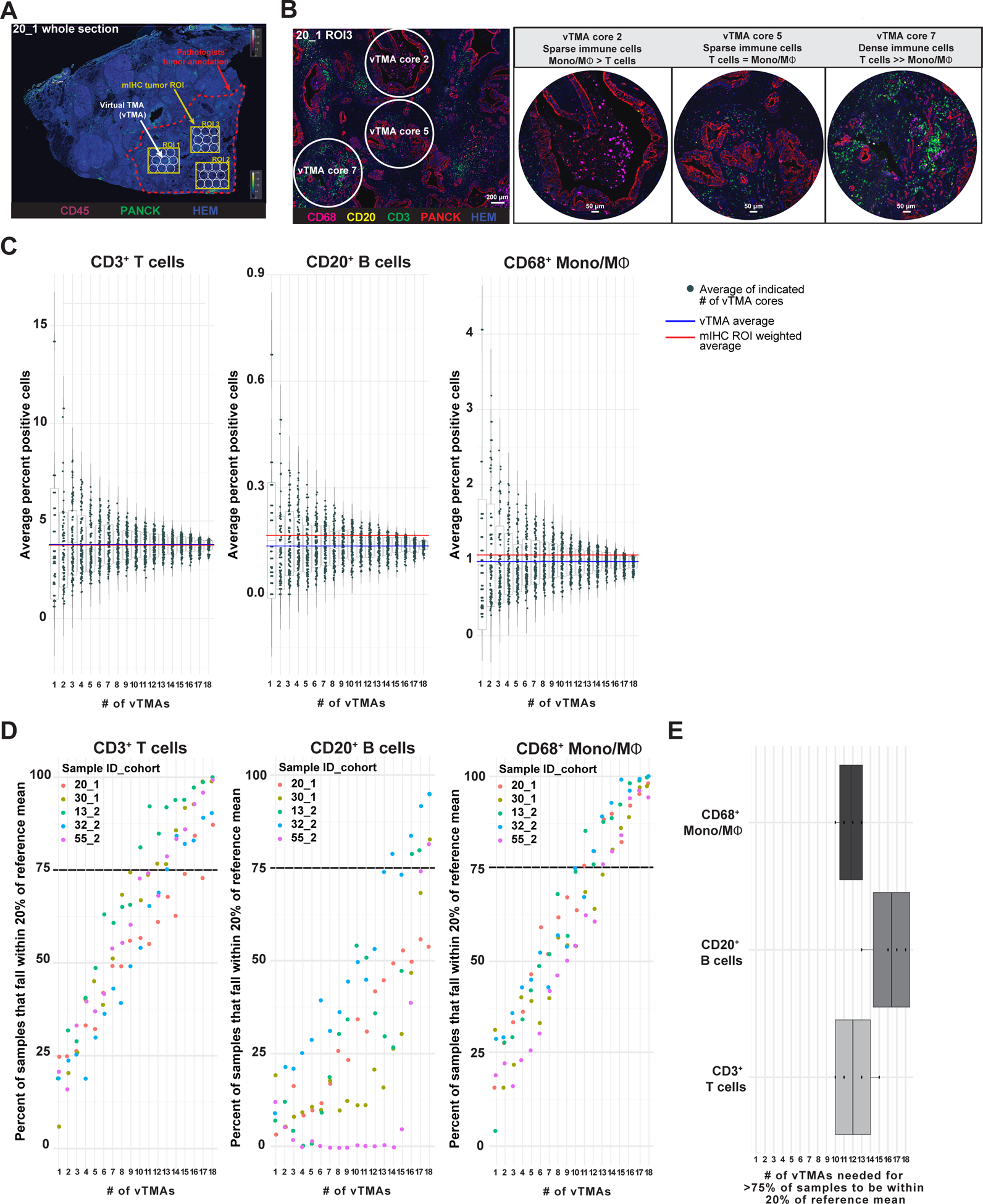
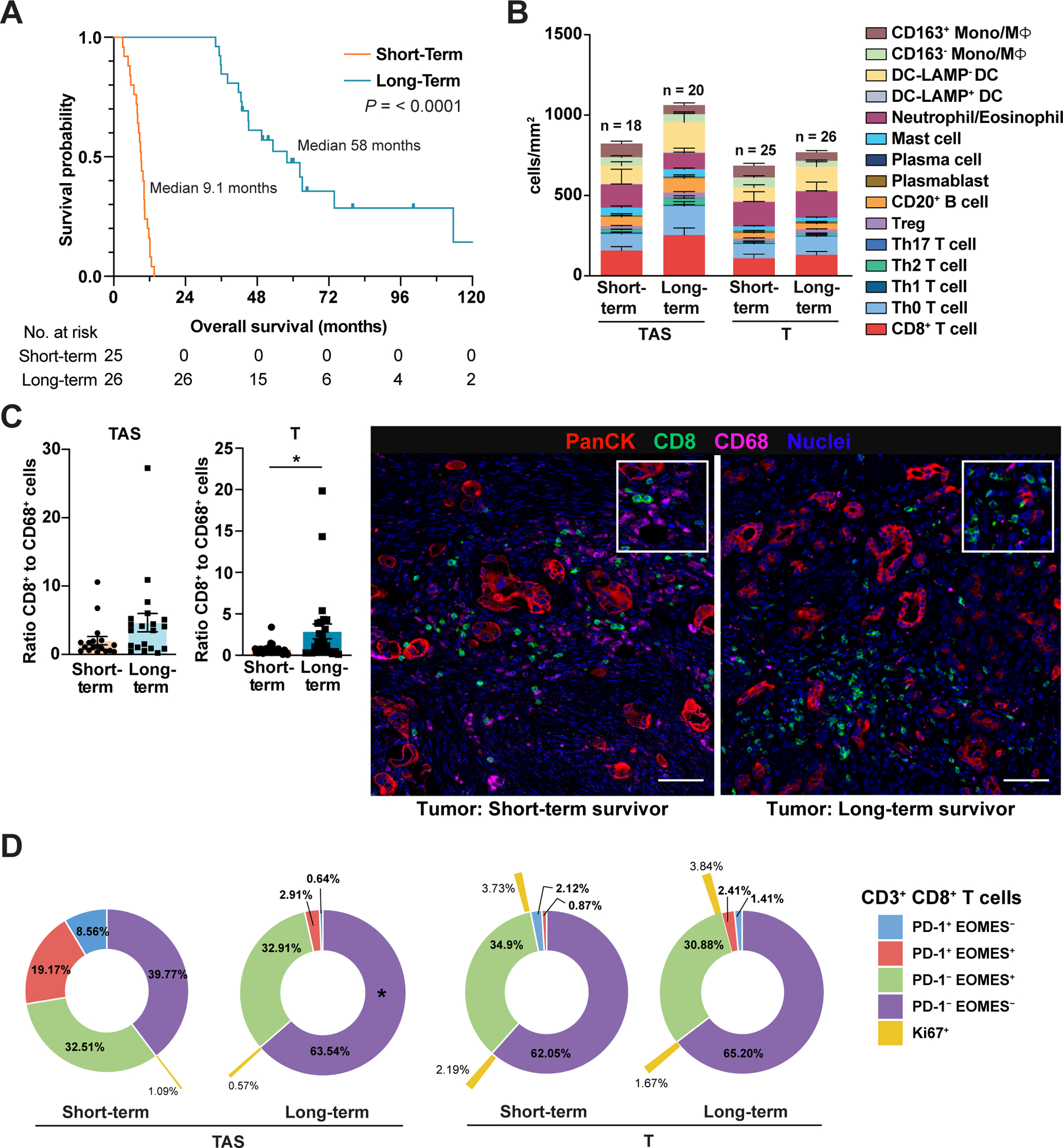
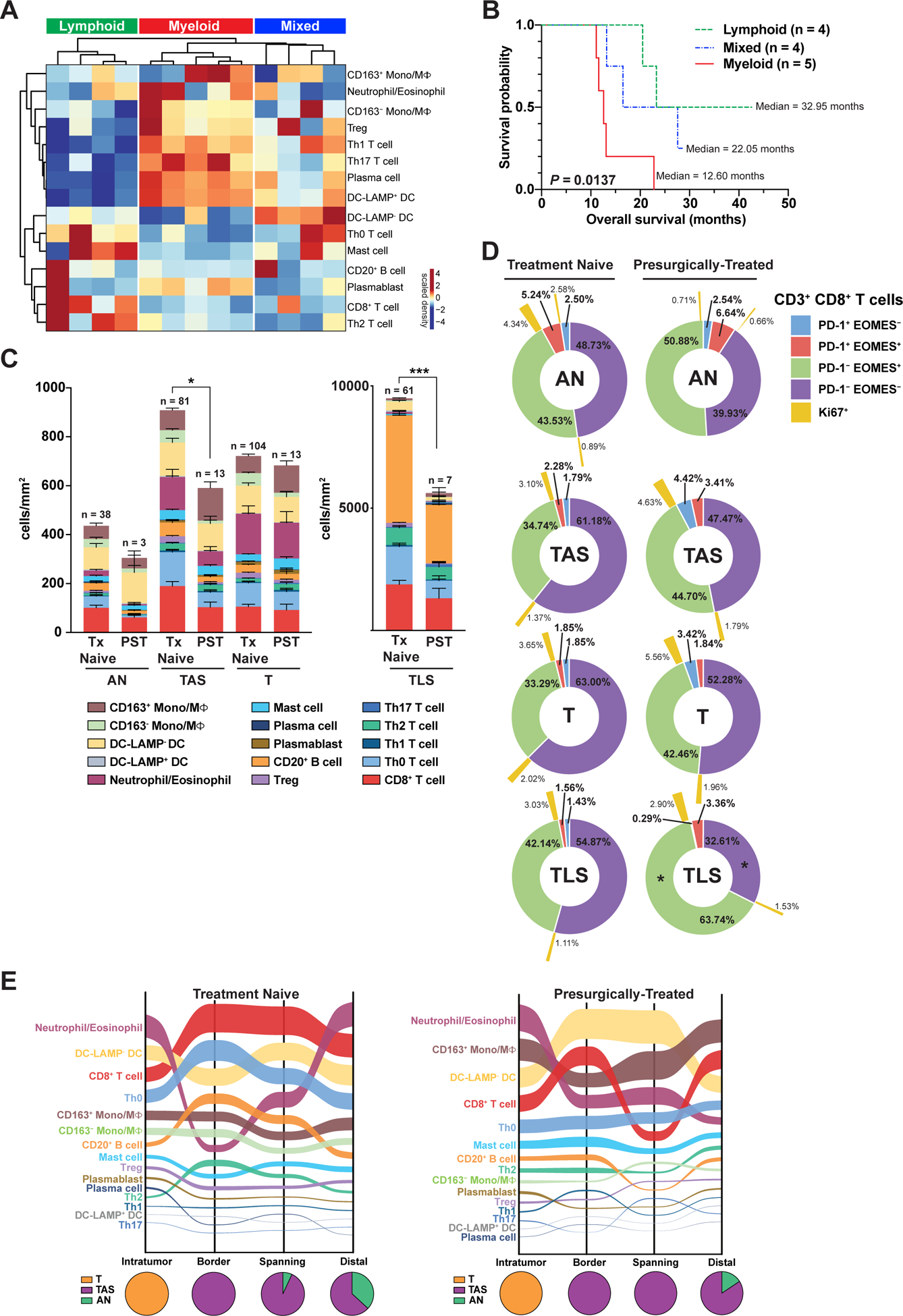
Immunotherapies targeting aspects of T cell functionality are efficacious in many solid tumors, but pancreatic ductal adenocarcinoma (PDAC) remains refractory to these treatments. Deeper understanding of the PDAC immune ecosystem is needed to identify additional therapeutic targets and predictive biomarkers for therapeutic response and resistance monitoring. To address these needs, we quantitatively evaluated leukocyte contexture in 135 human PDACs at single-cell resolution by profiling density and spatial distribution of myeloid and lymphoid cells within histopathologically defined regions of surgical resections from treatment-naive and presurgically (neoadjuvant)-treated patients and biopsy specimens from metastatic PDAC. Resultant data establish an immune atlas of PDAC heterogeneity, identify leukocyte features correlating with clinical outcomes, and, through an in silico study, provide guidance for use of PDAC tissue microarrays to optimally measure intratumoral immune heterogeneity. Atlas data have direct applicability as a reference for evaluating immune responses to investigational neoadjuvant PDAC therapeutics where pretherapy baseline specimens are not available. SIGNIFICANCE: We provide a phenotypic and spatial immune atlas of human PDAC identifying leukocyte composition at steady state and following standard neoadjuvant therapies. These data have broad utility as a resource that can inform on leukocyte responses to emerging therapies where baseline tissues were not acquired.This article is highlighted in the In This Issue feature, p. 1861.
©2021 American Association for Cancer Research.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
- R21 HD099367/HD/NICHD NIH HHS/United States
- U01 CA224012/CA/NCI NIH HHS/United States
- U01 CA210171/CA/NCI NIH HHS/United States
- P01 CA247886/CA/NCI NIH HHS/United States
- R01 CA223150/CA/NCI NIH HHS/United States
- U2C CA233280/CA/NCI NIH HHS/United States
- U54 CA209988/CA/NCI NIH HHS/United States
- R01 CA197296/CA/NCI NIH HHS/United States
- R01 CA226909/CA/NCI NIH HHS/United States
- R01 CA196228/CA/NCI NIH HHS/United States
- UL1 TR002369/TR/NCATS NIH HHS/United States
- U24 CA231877/CA/NCI NIH HHS/United States
- R01 CA186241/CA/NCI NIH HHS/United States
- P50 CA127003/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
