

ECG Changes in a Case of Posterior Myocardial Infarction in the Presence of Right Bundle Branch Block
- PMID: 33728214
- PMCID: PMC7949675
- DOI: 10.7759/cureus.13281
ECG Changes in a Case of Posterior Myocardial Infarction in the Presence of Right Bundle Branch Block
Abstract
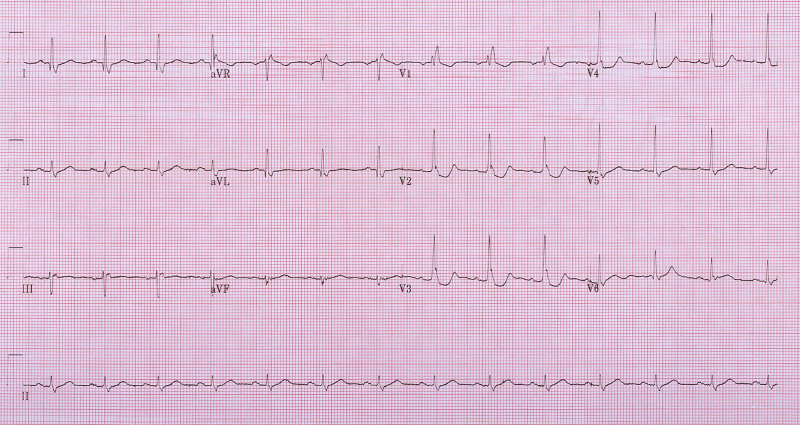
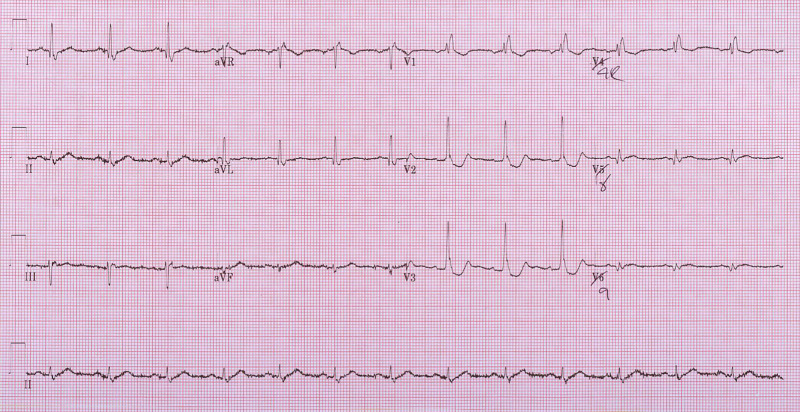
A 70-year-old male with hypertension and diabetes presented to the emergency department with a 1-hour history of chest pain. Initial 12-lead ECG revealed a right bundle branch block (RBBB) and ST depression (STD) in V2-V4. The anterior STD prompted a 15-lead ECG in which there was no evidence of ST elevation (STE). With a positive troponin, cardiology was consulted and the patient was admitted as a high-risk non-ST-elevation myocardial infarction (NSTEMI). Subsequently, his chest pain returned without further ST changes, regardless the patient went for emergency coronary angiography, which found a complete occlusion of the left circumflex artery. Anterior STD is a normal finding in RBBB and posterior STEs in the posterior leads are not always present making the recognition of posterior STEMI difficult. This case highlights three findings in leads V1-V3 that are concerning for posterior ischemia in the context of chest pain and an RBBB: tall R waves, upright T waves, and marked STD > 2 mm. This should prompt serial 15-lead ECGs and prompt cardiology consultation.
Keywords: cardiac electrophysiology; cardiology; emergency medicine; myocardial infarction.
Copyright © 2021, Ramjaun et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Posterior myocardial infarction and complete right bundle-branch block. Madias JE, Bravidis D, Attari M. Chest. 2002;122:1860–1864. - PubMed
-
- New electrocardiographic criteria for posterior wall acute myocardial ischemia validated by a percutaneous transluminal coronary angioplasty model of acute myocardial infarction. Wung SF, Drew BJ. Am J Cardiol. 2001;15:970–974. - PubMed
-
- ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to revise the 1999 guidelines for the management of patients with acute myocardial infarction) Antman EM, Anbe DT, Alpert JS, et al. J Am Coll Cardiol. 2004;44:0. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials